

Cardiac EASE (Ensuring Access and Speedy Evaluation) - the impact of a single-point-of-entry multidisciplinary outpatient cardiology consultation program on wait times in Canada
- PMID: 19960130
- PMCID: PMC2807832
- DOI: 10.1016/s0828-282x(09)70530-6
Cardiac EASE (Ensuring Access and Speedy Evaluation) - the impact of a single-point-of-entry multidisciplinary outpatient cardiology consultation program on wait times in Canada
Abstract
Background: Universal access to health care is valued in Canada but increasing wait times for services (eg, cardiology consultation) raise safety questions. Observations suggest that deficiencies in the process of care contribute to wait times. Consequently, an outpatient clinic was designed for Ensuring Access and Speedy Evaluation (Cardiac EASE) in a university group practice, providing cardiac consultative services for northern Alberta. Cardiac EASE has two components: a single-point-ofentry intake service (prospective testing using physician-approved algorithms and previsit triage) and a multidisciplinary clinic (staffed by cardiologists, nurse practitioners and doctoral-trained pharmacists).
Objectives: It was hypothesized that Cardiac EASE would reduce the time to initial consultation and a definitive diagnosis, and also increase the referral capacity.
Methods: The primary and secondary outcomes were time from referral to initial consultation, and time to achieve a definitive diagnosis and management plan, respectively. A conventionally managed historical control group (three-month pre-EASE period in 2003) was compared with the EASE group (2004 to 2006). The conventional referral mechanism continued concurrently with EASE.
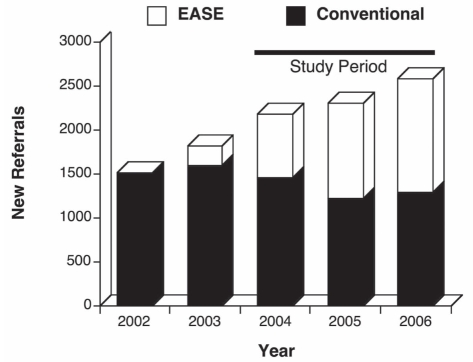
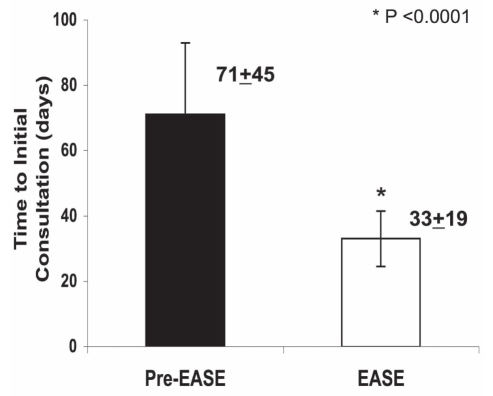
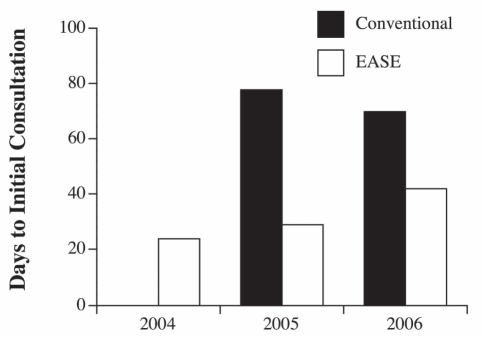
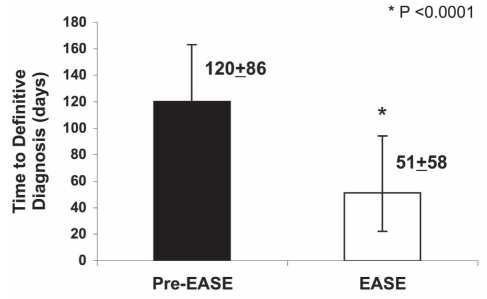
Results: A comparison between pre-EASE (n=311) and EASE (n=3096) revealed no difference in the mean (+/- SD) age (60+/-16 years), sex (55% and 52% men, respectively) or reason for referral, including chest pain (31% and 40%, respectively) and arrhythmia (27% and 29%, respectively). Cardiac EASE reduced the time to initial cardiac consultation (from 71+/-45 days to 33+/-19 days) and time to a definitive diagnosis (from 120+/-86 days to 51+/-58 days) (P<0.0001). The annual number of new referrals increased from 1512 in 2002 to 2574 in 2006 due to growth in the Cardiac EASE clinic. The number of patients seen through the conventional referral mechanism and their wait times remained constant during the study period.
Conclusions: Cardiac EASE reduced wait times, increased capacity and shortened time to achieve a diagnosis. The EASE model could shorten wait times for consultative services in Canada.
HISTORIQUE :: L’universalité des soins est un principe important au Canada, mais l’attente de plus en plus longue pour accéder aux services (p. ex., consultations en cardiologie) soulève des questions de sécurité. Selon certaines observations, des lacunes quant au déroulement des soins ne seraient pas étrangères aux temps d’attente. C’est pourquoi la clinique ambulatoire Cardiac EASE (Ensuring Access and Speedy Evaluation) a été mise sur pied dans une pratique de groupe universitaire offrant des services de consultations en cardiologie dans le Nord de l’Alberta. Le programme Cardiac EASE comporte deux volets : un service d’accès centralisé (analyses prospectives établies selon des algorithmes approuvés par les médecins et triage précédant la consultation) et une clinique pluridisciplinaire (offrant les services de cardiologues, d’infirmières praticiennes et de pharmaciens de niveau doctoral).
OBJECTIF :: Vérifier l’hypothèse selon laquelle le programme Cardiac EASE pourrait réduire le délai pour une consultation initiale et un diagnostic définitif, tout en accroissant la capacité de gérer les demandes de consultation.
MÉTHODES :: Les paramètres principal et secondaire étaient le délai entre la demande de consultation et la première consultation et le délai avant l’obtention d’un diagnostic définitif et d’un plan de traitement, respectivement. Un groupe témoin historique traité de la façon habituelle (période de trois mois précédant l’application du programme EASE en 2003) a été comparé au groupe EASE (de 2004 à 2006). Le processus habituel de demande de consultation a été maintenu pendant l’application du programme EASE.
RÉSULTATS :: Une comparaison entre les groupes pré-EASE (n = 311) et EASE (n = 3 096) n’a révélé aucune différence quant à l’âge moyen (± É. T.) (60 ± 16 ans), quant au sexe (55 % et 52 % d’hommes, respectivement) ou quant à la raison de la demande de consultation, soit DRS (31 % et 40 %, respectivement) et arythmie (27 % et 29 %, respectivement). Le programme Cardiac EASE a abrégé l’intervalle avant une première consultation en cardiologie (de 71 ± 45 jours à 33 ± 19 jours) et l’intervalle avant un diagnostic définitif (de 120 ± 86 jours à 51 ± 58 jours) (p < 0,0001). Le nombre annuel de nouvelles demandes de consultation est passé de 1 512 en 2002 à 2 574 en 2006 en raison de la croissance de la clinique Cardiac EASE. Le nombre de patients vus au moyen du processus habituel de demande de consultation et leurs temps d’attente sont demeurés constants pendant la durée de l’étude.
CONCLUSION :: Le programme Cardiac EASE a réduit les temps d’attente, augmenté le volume de patients et abrégé l’intervalle avant l’obtention du diagnostic. Le modèle EASE pourrait contribuer à abréger les temps d’attente pour l’accès aux services de consultation au Canada.
Figures
References
-
- Heart and Stroke Foundation of Canada Taking control: Lowering your risk of heart disease and stroke<ww2.heart&stroke.ca/PageID-1975&articleID-53317&Sfc-stroke&From-subCategory> (Version current at December 18, 2006).
-
- Capital Region Medical Staff Association Capital region physician access survey: Survey of wait times to access physician services (Physician Access Survey)<http://www.crmsa.ab.ca/Archives/cr_physician_access99.htm> (Survey Part 5, Version current at August 24, 2009).
-
- Teo KK, Spoor M, Pressey T, et al. Impact of managed waiting for coronary artery bypass graft surgery on patients’ perceived quality of life. Circ. 1998;98(19 Suppl):29–33. - PubMed
-
- Health Canada The Canada Health Act. 1984.
-
- Romanow RJ. Building on values: The future of health care in Canada final report. National Library of Canada. 2002.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
