

Cardiac adrenergic control and atrial fibrillation
- PMID: 19960186
- PMCID: PMC2855383
- DOI: 10.1007/s00210-009-0474-0
Cardiac adrenergic control and atrial fibrillation
Abstract
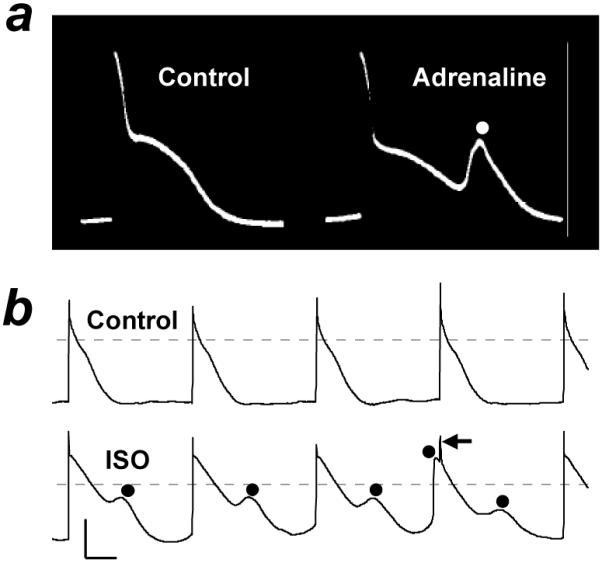
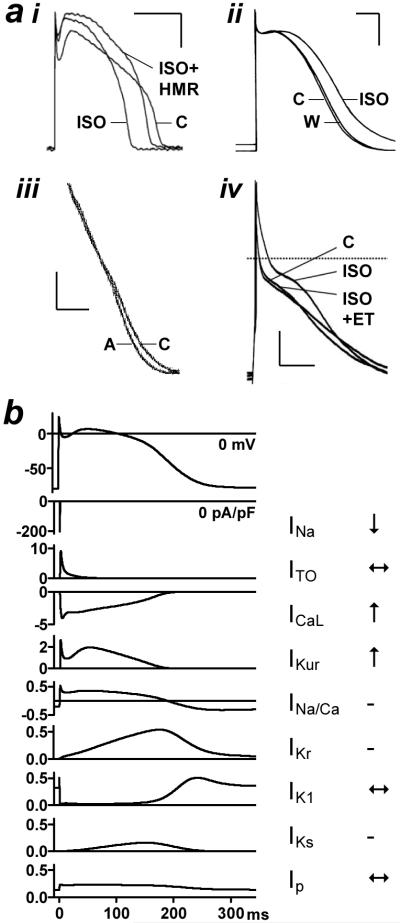
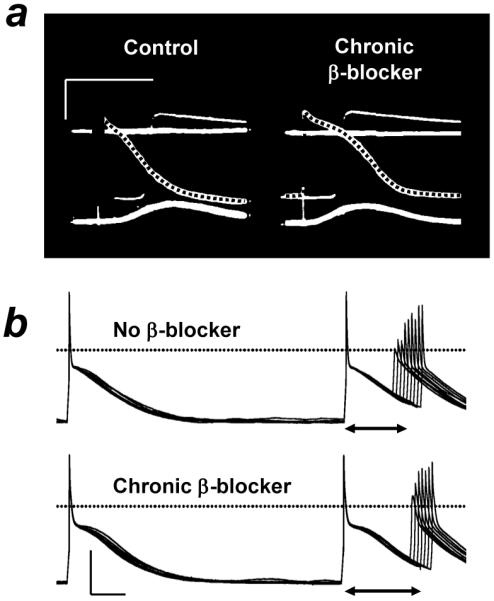
Atrial fibrillation (AF) is the most common cardiac arrhythmia, and it causes substantial mortality. The autonomic nervous system, and particularly the adrenergic/cholinergic balance, has a profound influence on the occurrence of AF. Adrenergic stimulation from catecholamines can cause AF in patients. In human atrium, catecholamines can affect each of the electrophysiological mechanisms of AF initiation and/or maintenance. Catecholamines may produce membrane potential oscillations characteristic of afterdepolarisations, by increasing Ca(2+) current, [Ca(2+)](i) and consequent Na(+)-Ca(2+) exchange, and may also enhance automaticity. Catecholamines might affect reentry, by altering excitability or conduction, rather than action potential terminal repolarisation or refractory period. However, which arrhythmia mechanisms predominate is unclear, and likely depends on cardiac pathology and adrenergic tone. Heart failure (HF), a major cause of AF, causes adrenergic activation and adaptational changes, remodelling, of atrial electrophysiology, Ca(2+) homeostasis, and adrenergic responses. Chronic AF also remodels these, but differently to HF. Myocardial infarction and AF cause neural remodelling that also may promote AF. beta-Adrenoceptor antagonists (beta-blockers) are used in the treatment of AF, mainly to control the ventricular rate, by slowing atrioventricular conduction. beta-Blockers also reduce the incidence of AF, particularly in HF or after cardiac surgery, when adrenergic tone is high. Furthermore, the chronic treatment of patients with beta-blockers remodels the atria, with a potentially antiarrhythmic increase in the refractory period. Therefore, the suppression of AF by beta-blocker treatment may involve an attenuation of arrhythmic activity that is caused by increased [Ca(2+)](i), coupled with effects of adaptation to the treatment. An improved understanding of the involvement of the adrenergic system and its control in basic mechanisms of AF under differing cardiac pathologies might lead to better treatments.
Figures
Similar articles
-
Effects of human atrial ionic remodelling by β-blocker therapy on mechanisms of atrial fibrillation: a computer simulation.Europace. 2014 Oct;16(10):1524-33. doi: 10.1093/europace/euu084. Epub 2014 Aug 1. Europace. 2014. PMID: 25085203 Free PMC article.
-
Chronic beta-adrenoceptor blockade and human atrial cell electrophysiology: evidence of pharmacological remodelling.Cardiovasc Res. 2003 Jun 1;58(3):518-25. doi: 10.1016/s0008-6363(03)00263-3. Cardiovasc Res. 2003. PMID: 12798424
-
Cellular bases for human atrial fibrillation.Heart Rhythm. 2008 Jun;5(6 Suppl):S1-6. doi: 10.1016/j.hrthm.2008.01.016. Epub 2008 Jan 17. Heart Rhythm. 2008. PMID: 18456193 Free PMC article.
-
Pharmacologic management of atrial fibrillation: current therapeutic strategies.Am Heart J. 2001 Feb;141(2 Suppl):S15-21. doi: 10.1067/mhj.2001.109952. Am Heart J. 2001. PMID: 11174354 Review.
-
Pharmacological approaches in the treatment of atrial fibrillation.Curr Med Chem. 2004 Jan;11(1):13-28. doi: 10.2174/0929867043456241. Curr Med Chem. 2004. PMID: 14754423 Review.
Cited by
-
Circadian Rhythms of Early Afterdepolarizations and Ventricular Arrhythmias in a Cardiomyocyte Model.Biophys J. 2021 Jan 19;120(2):319-333. doi: 10.1016/j.bpj.2020.11.2264. Epub 2020 Dec 5. Biophys J. 2021. PMID: 33285114 Free PMC article.
-
Accelerated atrial pacing reduces left-heart filling pressure: a combined clinical-computational study.Eur Heart J. 2024 Dec 7;45(46):4953-4964. doi: 10.1093/eurheartj/ehae718. Eur Heart J. 2024. PMID: 39589540 Free PMC article.
-
Long Non-coding RNA Involved in the Pathophysiology of Atrial Fibrillation.Cardiovasc Drugs Ther. 2025 Apr;39(2):435-458. doi: 10.1007/s10557-023-07491-8. Epub 2023 Sep 13. Cardiovasc Drugs Ther. 2025. PMID: 37702834 Free PMC article. Review.
-
Chronic myocardial infarction promotes atrial action potential alternans, afterdepolarizations, and fibrillation.Cardiovasc Res. 2013 Jul 1;99(1):215-24. doi: 10.1093/cvr/cvt087. Epub 2013 Apr 8. Cardiovasc Res. 2013. PMID: 23568957 Free PMC article.
-
Enhanced Cardiac CaMKII Oxidation and CaMKII-Dependent SR Ca Leak in Patients with Sleep-Disordered Breathing.Antioxidants (Basel). 2022 Feb 8;11(2):331. doi: 10.3390/antiox11020331. Antioxidants (Basel). 2022. PMID: 35204213 Free PMC article.
References
-
- Barbuti A, Terragni B, Brioschi C, et al. Localization of f-channels to caveolae mediates specific β2-adrenergic receptor modulation of rate in sinoatrial myocytes. J Mol Cell Cardiol. 2007;42:71–78. - PubMed
-
- Bartholomeu JB, Vanzelli AS, Rolim NPL, et al. Intracellular mechanisms of specific beta-adrenoceptor antagonists involved in improved cardiac function and survival in a genetic model of heart failure. J Mol Cell Cardiol. 2008;45:240–249. - PubMed
-
- Bers DM. Cardiac excitation-contraction coupling. Nature. 2002;415:198–205. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
