

Impaired beta-cell sensitivity to glucose and maximal insulin secretory capacity in adolescents with type 2 diabetes
- PMID: 19961550
- PMCID: PMC3761801
- DOI: 10.1111/j.1399-5448.2009.00601.x
Impaired beta-cell sensitivity to glucose and maximal insulin secretory capacity in adolescents with type 2 diabetes
Abstract
Background: Adults with type 2 diabetes mellitus (T2DM) have broad impairments in beta-cell function, including severe attenuation of the first-phase insulin response to glucose, and reduced beta-cell mass. In adolescents with T2DM, there is some evidence that beta-cell dysfunction may be less severe. Our objective was to determine beta-cell sensitivity to glucose and maximal insulin secretory capacity (AIR(max)) in teenagers with T2DM.
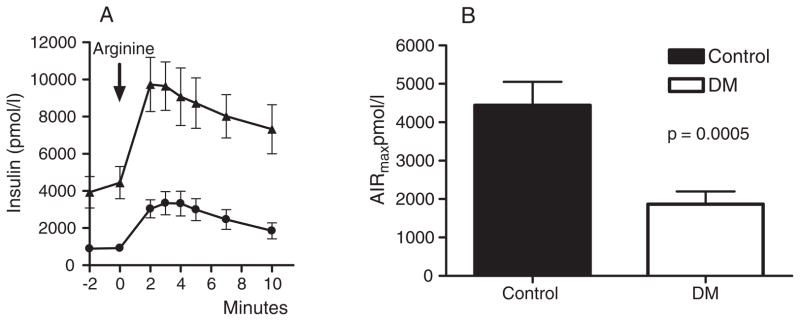
Methods: Fifteen adolescents with T2DM [11 F/4 M, age 18.4 +/- 0.3 yr, body mass index (BMI) 39.8 +/- 2.2 kg/m(2)] and 10 non-diabetic control subjects (7 F/3 M, age 17.4 +/- 0.5 yr, BMI 41.5 +/- 2.2 kg/m(2)) were studied. T2DM subjects had a mean duration of diabetes of 48.8 +/- 6.4 months, were treated with conventional therapies, and had good metabolic control [hemoglobin A1c (HbA1c) 6.7 +/- 1.2%]. Insulin and C-peptide were determined before and after a graded glucose infusion and after intravenous arginine at a whole blood glucose level of >or=22 mM.
Results: The insulin response to increasing plasma glucose concentrations was blunted in the diabetic compared with control subjects (34.8 +/- 11.9 vs. 280.5 +/- 57.8 pmol/mmol; p < 0.0001), and AIR(max) was also significantly reduced in the diabetic group (1868 +/- 330 vs. 4445 +/- 606; p = 0.0005).
Conclusion: Even adolescents with well-controlled T2DM have severe impairments of insulin secretion. These data support beta-cell dysfunction as central in the pathogenesis of T2DM in young people, and indicate that these abnormalities can develop over a period of just several years.
Figures


References
-
- Hannon TS, Rao G, Arslanian SA. Childhood obesity and type 2 diabetes mellitus. Pediatrics. 2005;116:473–480. - PubMed
-
- Bobo N, Evert A, Gallivan J, et al. An update on type 2 diabetes in youth from the National Diabetes Education Program. Pediatrics. 2004;114:259–263. - PubMed
-
- Duncan GE. Prevalence of diabetes and impaired fasting glucose levels among US adolescents: National Health and Nutrition Examination Survey, 1999–2002. Arch Pediatr Adolesc Med. 2006;160:523–528. - PubMed
-
- Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. Jama. 2004;291:2847–2850. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. Jama. 2006;295:1549–1555. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
