

Vacuum-assisted closure device enhances recovery of critically ill patients following emergency surgical procedures
- PMID: 19961614
- PMCID: PMC2811940
- DOI: 10.1186/cc8193
Vacuum-assisted closure device enhances recovery of critically ill patients following emergency surgical procedures
Abstract
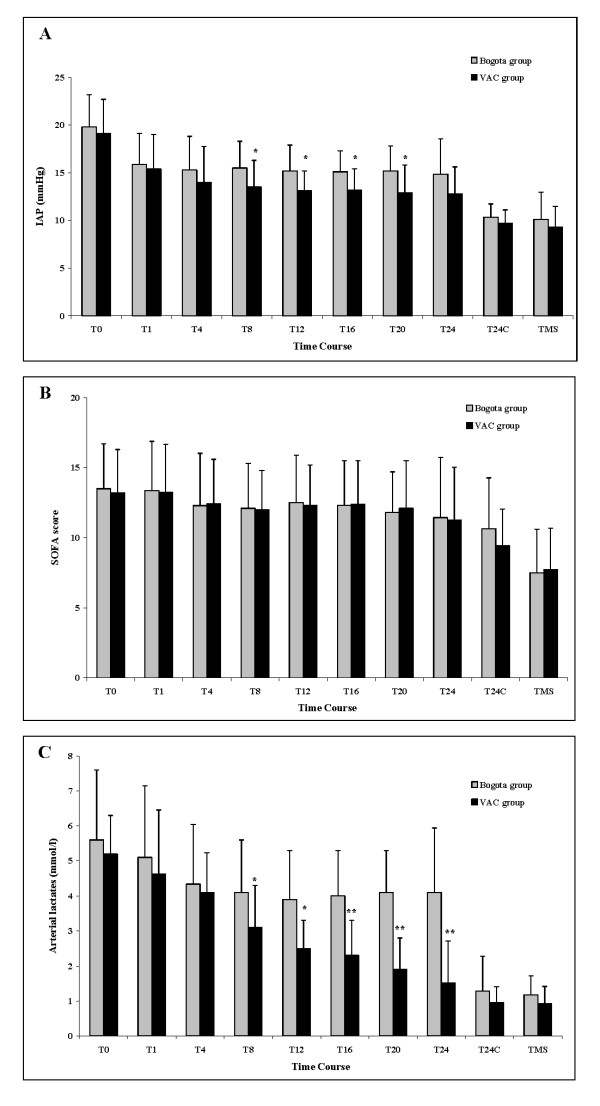
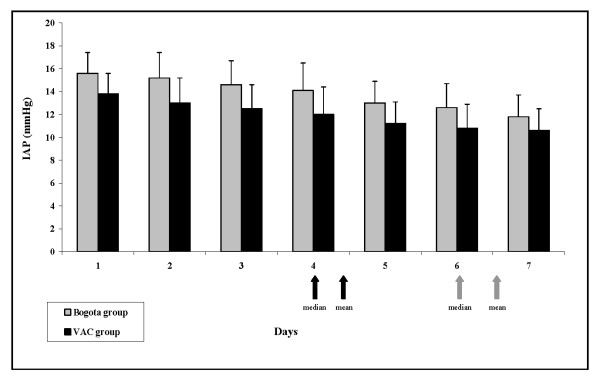
Introduction: Critically ill surgical patients frequently develop intra-abdominal hypertension (IAH) leading to abdominal compartment syndrome (ACS) with subsequent high mortality. We compared two temporary abdominal closure systems (Bogota bag and vacuum-assisted closure (VAC) device) in intra-abdominal pressure (IAP) control.
Methods: This prospective study with a historical control included 66 patients admitted to a medical and surgical intensive care unit (ICU) of a tertiary care referral center (Careggi Hospital, Florence, Italy) from January 2006 to April 2009. The control group included patients consecutively treated with the Bogota bag (Jan 2006-Oct 2007), whereas the prospective group was comprised of patients treated with a VAC. All patients underwent abdominal decompressive surgery. Groups were compared based upon their IAP, SOFA score, serial arterial lactates, the duration of having their abdomen open, the need for mechanical ventilation (MV) along with length of ICU and hospital stay and mortality. Data were collected from the time of abdominal decompression until the end of pressure monitoring.
Results: The Bogota and VAC groups were similar with regards to demography, admission diagnosis, severity of illness, and IAH grading. The VAC system was more effective in controlling IAP (P < 0.01) and normalizing serum lactates (P < 0.001) as compared to the Bogota bag during the first 24 hours after surgical decompression. There was no significant difference between the SOFA scores. When compared to the Bogota, the VAC group had a faster abdominal closure time (4.4 vs 6.6 days, P = 0.025), shorter duration of MV (7.1 vs 9.9 days, P = 0.039), decreased ICU length of stay (LOS) (13.3 vs 19.2 days, P = 0.024) and hospital LOS (28.5 vs 34.9 days; P = 0.019). Mortality rate did not differ significantly between the two groups.
Conclusions: Patients with abdominal compartment syndrome who were treated with VAC decompression had a faster abdominal closure rate and earlier discharge from the ICU as compared to similar patients treated with the Bogota bag.
Figures
Comment in
-
Prophylactic open abdomen in patients with postoperative intra-abdominal hypertension.Crit Care. 2010;14(1):111. doi: 10.1186/cc8207. Epub 2010 Feb 4. Crit Care. 2010. PMID: 20156323 Free PMC article.
-
Vacuum-assisted closure device in intensive care unit patients and dissemination of Gram-negative bacteria.Crit Care. 2010;14(2):413. doi: 10.1186/cc8944. Epub 2010 Apr 19. Crit Care. 2010. PMID: 20429958 Free PMC article.
Similar articles
-
Comparison of early surgical alternatives in the management of open abdomen: a randomized controlled study.Ulus Travma Acil Cerrahi Derg. 2015 May;21(3):168-74. doi: 10.5505/tjtes.2015.09804. Ulus Travma Acil Cerrahi Derg. 2015. PMID: 26033648 Clinical Trial.
-
Intra-abdominal pressure development after different temporary abdominal closure techniques in a porcine model.J Trauma. 2009 Apr;66(4):1118-24. doi: 10.1097/TA.0b013e3181820d94. J Trauma. 2009. PMID: 19359923
-
Intra-abdominal pressure may be elevated in patients with open abdomen after emergent laparotomy.Langenbecks Arch Surg. 2020 Feb;405(1):91-96. doi: 10.1007/s00423-020-01854-7. Epub 2020 Jan 18. Langenbecks Arch Surg. 2020. PMID: 31955259
-
Increased pressure within the abdominal compartment: intra-abdominal hypertension and the abdominal compartment syndrome.Curr Opin Crit Care. 2016 Apr;22(2):174-85. doi: 10.1097/MCC.0000000000000289. Curr Opin Crit Care. 2016. PMID: 26844989 Review.
-
Vacuum-assisted closure or primary closure with relaparotomy on-demand in patients with secondary peritonitis: a systematic review and meta-analysis.World J Emerg Surg. 2025 May 22;20(1):42. doi: 10.1186/s13017-025-00615-5. World J Emerg Surg. 2025. PMID: 40399929 Free PMC article. Review.
Cited by
-
Negative pressure wound therapy management of the "open abdomen" following trauma: a prospective study and systematic review.World J Emerg Surg. 2013 Jan 10;8(1):4. doi: 10.1186/1749-7922-8-4. World J Emerg Surg. 2013. PMID: 23305306 Free PMC article.
-
Successful Use of Negative Pressure Wound Therapy for Abdominal Wall Necrosis Caused by a Perforated Ascending Colon Using the ABThera System.Case Rep Surg. 2020 Jul 21;2020:8833566. doi: 10.1155/2020/8833566. eCollection 2020. Case Rep Surg. 2020. PMID: 32774978 Free PMC article.
-
Abdominal negative-pressure therapy: a new method in countering abdominal compartment and peritonitis - prospective study and critical review of literature.Ann Intensive Care. 2012 Dec 20;2 Suppl 1(Suppl 1):S23. doi: 10.1186/2110-5820-2-S1-S23. Epub 2012 Dec 20. Ann Intensive Care. 2012. PMID: 23281649 Free PMC article.
-
Prophylactic open abdomen in patients with postoperative intra-abdominal hypertension.Crit Care. 2010;14(1):111. doi: 10.1186/cc8207. Epub 2010 Feb 4. Crit Care. 2010. PMID: 20156323 Free PMC article.
-
Abdominal and thoracic wall closure: damage control surgery's cinderella.Colomb Med (Cali). 2021 Jun 30;52(2):e4144777. doi: 10.25100/cm.v52i2.4777. eCollection 2021 Apr-Jun. Colomb Med (Cali). 2021. PMID: 34908622 Free PMC article. Review.
References
-
- Malbrain ML, Cheatham ML, Kirkpatrick A, Sugrue M, Parr M, De Waele J, Balogh Z, Leppaniemi A, Olvera C, Ivatury R, D'Amours S, Wendon J, Hillman K, Johansson K, Kolkman K, Wilmer A. Results from the International Conference of Experts on Intra-abdominal Hypertension and Abdominal Compartment Syndrome. I. Definitions. Intensive Care Med. 2006;32:1722–1732. doi: 10.1007/s00134-006-0349-5. - DOI - PubMed
-
- Malbrain ML, Vidts W, Ravyts M, De Laet I, De Waele J. Acute intestinal distress syndrome: the importance of intra-abdominal pressure. Minerva Anestesiol. 2008;74:657–673. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
