

Pharyngeal airway volume and shape from cone-beam computed tomography: relationship to facial morphology
- PMID: 19962603
- PMCID: PMC2891076
- DOI: 10.1016/j.ajodo.2008.01.020
Pharyngeal airway volume and shape from cone-beam computed tomography: relationship to facial morphology
Abstract
Introduction: The aim of this study was to assess the differences in airway shape and volume among subjects with various facial patterns.
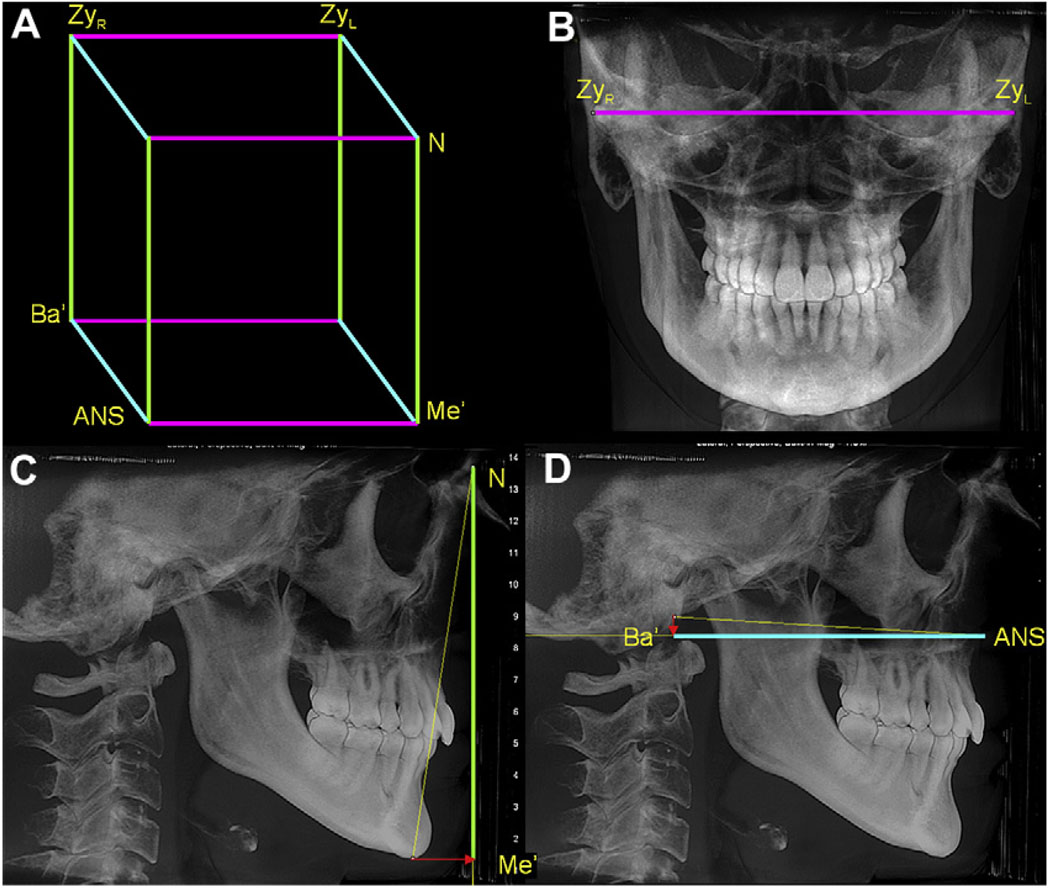
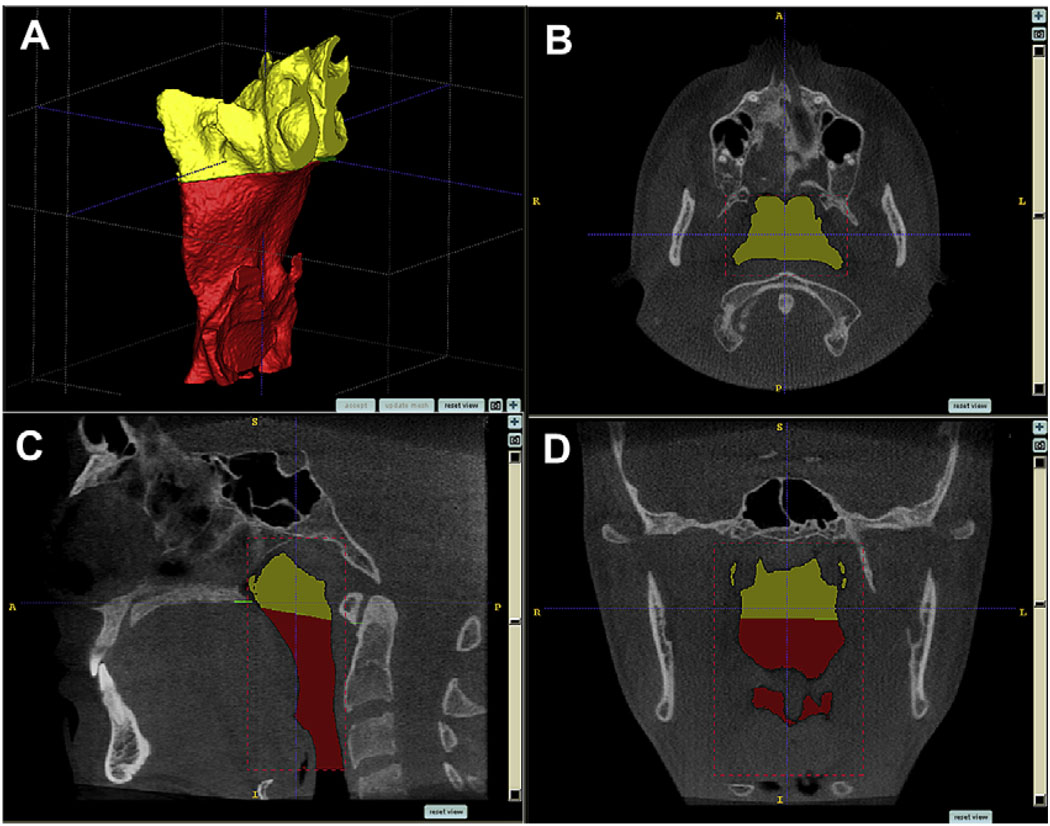
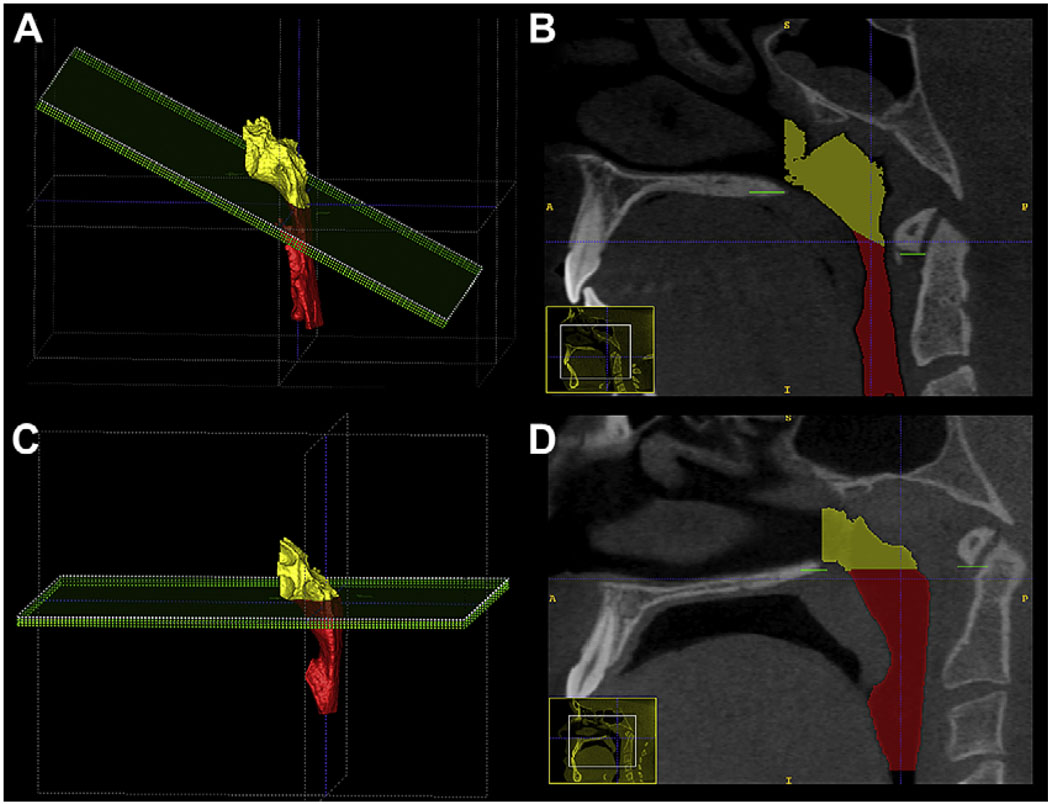
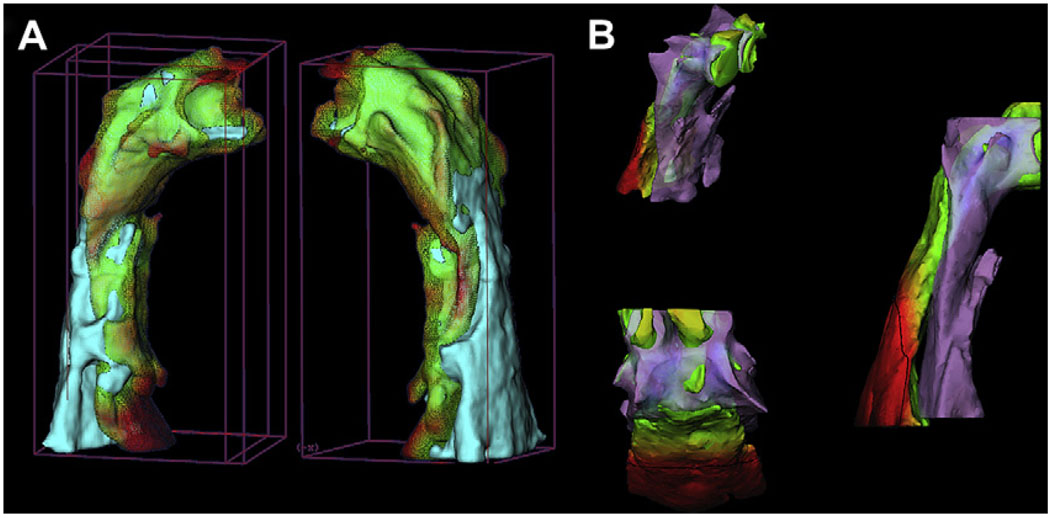
Methods: Cone-beam computed tomography records of 62 nongrowing patients were used to evaluate the pharyngeal airway volume (superior and inferior compartments) and shape. This was done by using 3-dimensional virtual surface models to calculate airway volumes instead of estimates based on linear measurements. Subgroups of the sample were determined by anteroposterior jaw relationships and vertical proportions.
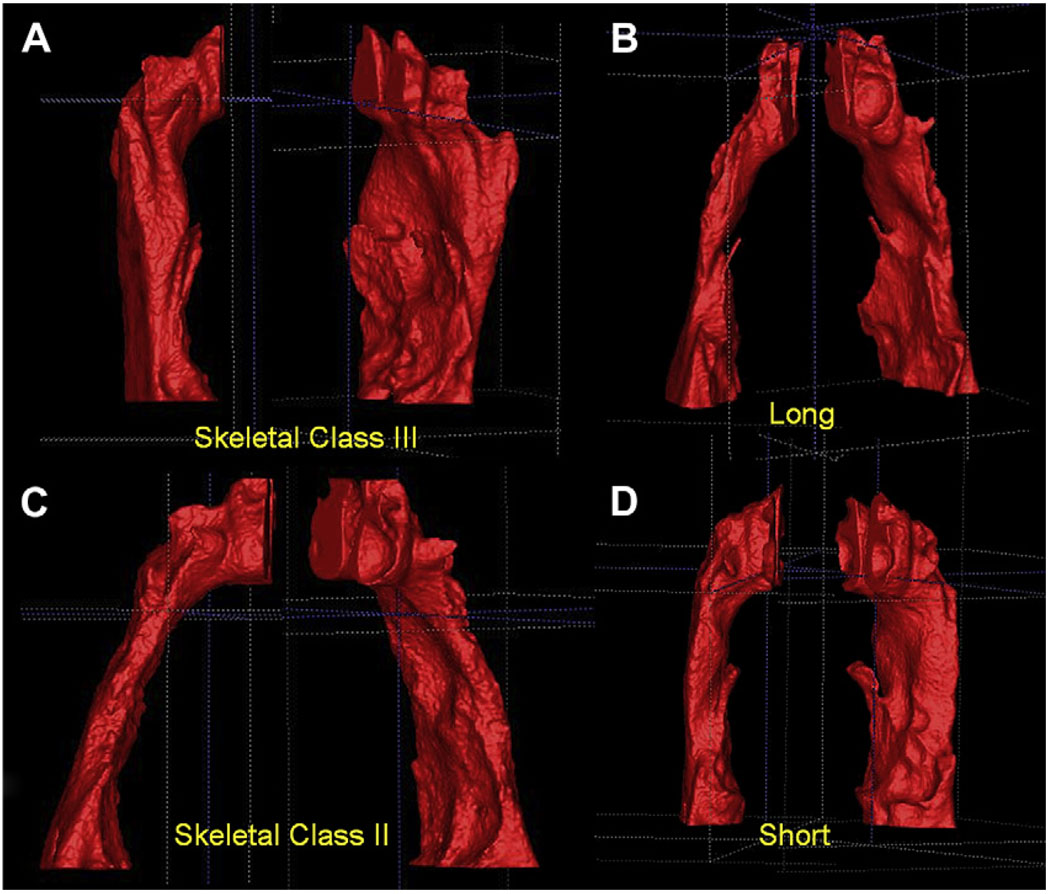
Results: There was a statistically significant relationship between the volume of the inferior component of the airway and the anteroposterior jaw relationship (P = 0.02), and between airway volume and both size of the face and sex (P = 0.02, P = 0.01). No differences in airway volumes related to vertical facial proportions were found. Skeletal Class II patients often had forward inclination of the airway (P <0.001), whereas skeletal Class III patients had a more vertically oriented airway (P = 0.002).
Conclusions: Airway volume and shape vary among patients with different anteroposterior jaw relationships; airway shape but not volume differs with various vertical jaw relationships. The methods developed in this study make it possible to determine the relationship of 3-dimensional pharyngeal airway surface models to facial morphology, while controlling for variability in facial size.
Figures

References
-
- Linder-Aronson S. Adenoids. Their effect on mode of breathing and nasal airflow and their relationship to characteristics of the facial skeleton and the dentition. A biometric rhino-manometric and cephalometro-radiographic study on children with and without adenoids. Acta Otolaryngol Suppl. 1970;265:1–132. - PubMed
-
- Linder-Aronson S, Woodside DG, Lundstrom A. Mandibular growth direction following adenoidectomy. Am J Orthod. 1986;89:273–284. - PubMed
-
- McNamara JA. Influence of respiratory pattern on craniofacial growth. Angle Orthod. 1981;51:269–300. - PubMed
-
- Zettergren-Wijk L, Forsberg CM, Linder-Aronson S. Changes in dentofacial morphology after adeno-tonsillectomy in young children with obstructive sleep apnoea—a 5-year follow-up study. Eur J Orthod. 2006;28:319–326. - PubMed
-
- Guray E, Karaman AI. Effects of adenoidectomy on dentofacial structures: a 6-year longitudinal study. World J Orthod. 2002;3:73–81.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
