

Individualized therapy to prevent bone mineral density loss after kidney and kidney-pancreas transplantation
- PMID: 19965527
- PMCID: PMC2801646
- DOI: 10.2215/CJN.03770609
Individualized therapy to prevent bone mineral density loss after kidney and kidney-pancreas transplantation
Abstract
Background and objectives: Most patients who undergo kidney or kidney-pancreas transplantation have renal osteodystrophy, and immediately after transplantation bone mineral density (BMD) commonly falls. Together, these abnormalities predispose to an increased fracture incidence. Bisphosphonate or calcitriol therapy can preserve BMD after transplantation, but although bisphosphonates may be more effective, they pose potential risks for adynamic bone.
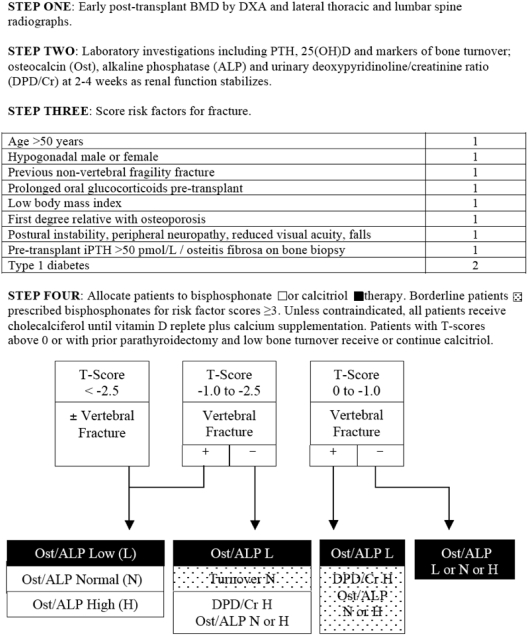
Design, setting, participants, & measurements: A total of 153 kidney (61%) and kidney-pancreas (39%) transplant recipients were allocated to bisphosphonate (62%) or calcitriol (38%) therapy using an algorithm that incorporated BMD, prevalent vertebral fracture, biomarkers of bone turnover, and risk factor assessment. Patients received cholecalciferol and calcium as appropriate and were followed for 12 mo.
Results: Patients who were treated with bisphosphonates had lower BMD at the lumbar spine and femoral neck and longer time on dialysis. Age and gender were similar between the groups. At 12 mo, bisphosphonate-treated patients had significant BMD increases at the lumber spine and femoral neck and a negative trend at the wrist. Patients who were allocated to calcitriol, who were assessed to have lower baseline fracture risk, had no significant change in BMD at any site. At 1 yr, mean levels of bone turnover marker and intact parathyroid hormone normalized in both groups. Incident fracture rates did not differ significantly.
Conclusions: With targeted treatment, BMD levels were stable or improved and bone turnover markers normalized. This algorithm provides a guide to targeting therapy after transplantation that avoids BMD loss and may reduce suppression of bone turnover.
Figures
References
-
- Coco M, Rush H: Increased incidence of hip fractures in dialysis patients with low serum parathyroid hormone. Am J Kidney Dis 36: 1115–1121, 2000 - PubMed
-
- Elder G, Mackun K: 25-Hydroxyvitamin D deficiency and diabetes predict reduced bone mineral density in patients with chronic kidney disease. J Bone Miner Res 21: 1778–1784, 2006 - PubMed
-
- Monier-Faugere MC, Mawad H, Qi Q, Friedler RM, Malluche HH: High prevalence of low bone turnover and occurrence of osteomalacia after kidney transplantation. J Am Soc Nephrol 11: 1093–1099, 2000 - PubMed
-
- Rojas E, Carlini R, Clesca P, Arminio A, Suniaga O, Elguezabal K, Weisinger J, Hruska K, Bellorin-Font E: The pathogenesis of osteodystrophy after renal transplantation as detected by early alterations in bone remodeling. Kidney Int 63: 1915–1923, 2003 - PubMed
-
- Casez JP, Lippuner K, Horber FF, Montandon A, Jaeger P: Changes in bone mineral density over 18 months following kidney transplantation: The respective roles of prednisone and parathyroid hormone. Nephrol Dial Transplant 17: 1318–1326, 2002 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
