

Longitudinal relationships among coronary artery calcification, serum phosphorus, and kidney function
- PMID: 19965546
- PMCID: PMC2798869
- DOI: 10.2215/CJN.01250209
Longitudinal relationships among coronary artery calcification, serum phosphorus, and kidney function
Abstract
Background and objectives: Coronary artery calcification (CAC) is common in advanced chronic kidney disease (CKD), yet its onset and time course are uncertain. The study objective was to assess longitudinal relationships among CAC, kidney function, and traditional and putative cardiovascular disease (CVD) risk factors.
Design, setting, participants, & measurements: This is a prospective cohort analysis from the Spokane Heart Study, a long-term observational study of community-dwelling adults who were assessed every 2 yr for CAC (electron-beam computed tomography), CVD risk factors, and laboratory testing. Estimated GFR (eGFR) was determined by the reexpressed Modification of Diet in Renal Disease equation.
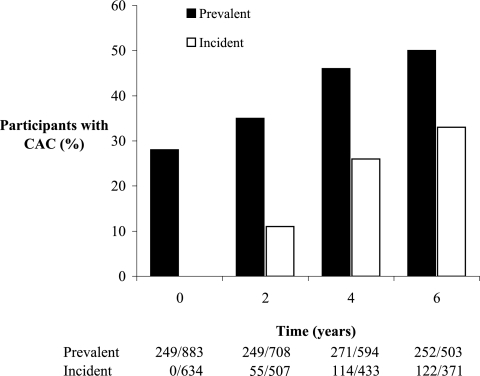
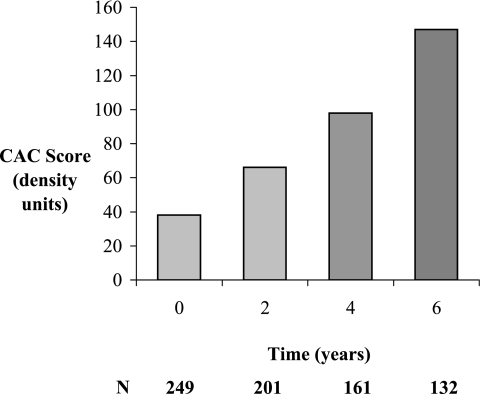
Results: CAC was present in 28% (245 of 883) at baseline. After 6 yr, new-onset CAC developed in 33% (122 of 371); severity increased from a median CAC score of 38 to 152 in those with baseline CAC. Neither eGFR (101 +/- 34 versus 104 +/- 31 ml/min per 1.73 m(2), respectively) nor serum phosphorus (3.25 +/- 0.49 versus 3.29 +/- 0.48 mg/dl, respectively) differed by CAC presence or absence at baseline; however, multivariate models (generalized estimating equations for incidence and prevalence) revealed that independent predictors of CAC over time were greater baseline CAC scores, higher serum phosphorus levels, lower eGFR levels, and traditional CVD risk factors. Each 1-mg/dl increase in phosphorus imparted odds ratios for CAC of 1.61 (incidence) and 1.54 (prevalence), risks comparable to traditional CVD risk factors.
Conclusions: CAC becomes more frequent and severe over time. Higher levels of serum phosphorus and reduced kidney function independently predicted CAC.
Figures
Comment in
-
Coronary calcification in chronic kidney disease: morphology, mechanisms and mortality.Clin J Am Soc Nephrol. 2009 Dec;4(12):1883-5. doi: 10.2215/CJN.07611009. Epub 2009 Nov 19. Clin J Am Soc Nephrol. 2009. PMID: 19965543 No abstract available.
References
-
- Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX: Chronic kidney disease and mortality risk: A systematic review. J Am Soc Nephrol 17: 2034–2047, 2006 - PubMed
-
- Go AS, Chertow GM, Fan D, McCullough CE, Hsu C-Y: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RRUKPDS Group: Development and progression of nephropathy in type 2 diabetes: The United Kingdom prospective diabetes study (UKPDS 64). Kidney Int 63: 225–232, 2003 - PubMed
-
- Raggi P, Boulay A, Chasan-Taber S, Amin N, Dillon M, Burke SK, Chertow GM: Cardiac calcification in adult hemodialysis patients: A link between end-stage renal disease and cardiovascular disease? J Am Coll Cardiol 39: 695–701, 2002 - PubMed
-
- Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB: Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 342: 1478–1483, 2000 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
