

Bone regeneration in defects compromised by radiotherapy
- PMID: 19966040
- PMCID: PMC2798583
- DOI: 10.1177/0022034509352151
Bone regeneration in defects compromised by radiotherapy
Abstract
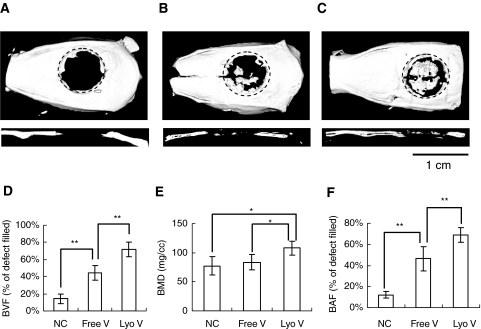
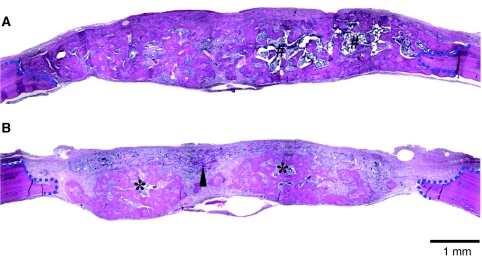
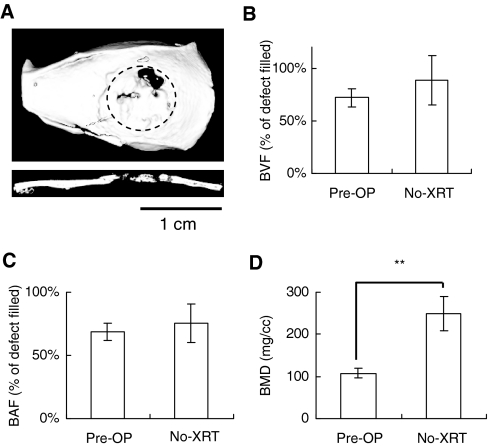
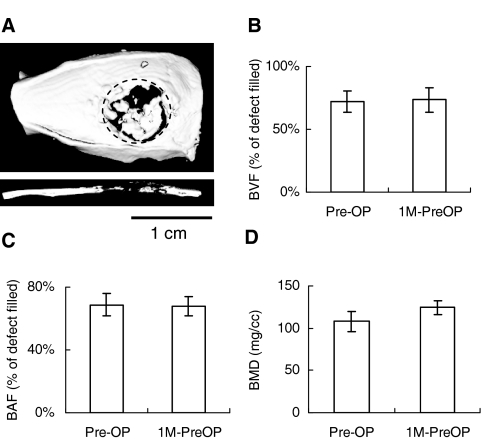
Because bone reconstruction in irradiated sites is less than ideal, we applied a regenerative gene therapy method in which a cell-signaling virus was localized to biomaterial scaffolds to regenerate wounds compromised by radiation therapy. Critical-sized defects were created in rat calvariae previously treated with radiation. Gelatin scaffolds containing lyophilized adenovirus encoding BMP-2 (AdBMP-2) or freely suspended AdBMP-2 were transplanted. Lyophilized AdBMP-2 significantly improved bone quality and quantity over free AdBMP-2. Bone mineral density was reduced after radiotherapy. Histological analyses demonstrated that radiation damage led to less bone regeneration. The woven bone and immature marrow formed in the radiated defects indicated that irradiation retarded normal bone development. Finally, we stored the scaffolds with lyophilized AdBMP-2 at -80 degrees C to determine adenovirus stability. Micro-CT quantification demonstrated no significant differences between bone regeneration treated with lyophilized AdBMP-2 before and after storage, suggesting that virus-loaded scaffolds may be convenient for application as pre-made constructs.
Figures
References
-
- Chang SC, Wei FC, Chuang HL, Chen YR, Chen JK, Lee KC, et al. (2003). Ex vivo gene therapy in autologous critical-size craniofacial bone regeneration. Plast Reconstr Surg 112:1841-1850 - PubMed
-
- Deutsch M, Kroll SS, Ainsle N, Wang B. (1999). Influence of radiation on late complications in patients with free fibular flaps for mandibular reconstruction. Ann Plast Surg 42:662-664 - PubMed
-
- Disa JJ, Cordeiro PG. (2000). Mandible reconstruction with microvascular surgery. Semin Surg Oncol 19:226-234 - PubMed
-
- Ehrhart NP, Hong L, Morgan AL, Eurell JA, Jamison RD. (2005). Effect of transforming growth factor-beta1 on bone regeneration in critical-sized bone defects after irradiation of host tissues. Am J Vet Res 66:1039-1045 - PubMed
-
- Emerick KS, Teknos TN. (2007). State-of-the-art mandible reconstruction using revascularized free-tissue transfer. Expert Rev Anticancer Ther 7:1781-1788 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
