

Acute stroke magnetic resonance imaging: current status and future perspective
- PMID: 19967531
- PMCID: PMC8177054
- DOI: 10.1007/s00234-009-0637-1
Acute stroke magnetic resonance imaging: current status and future perspective
Abstract
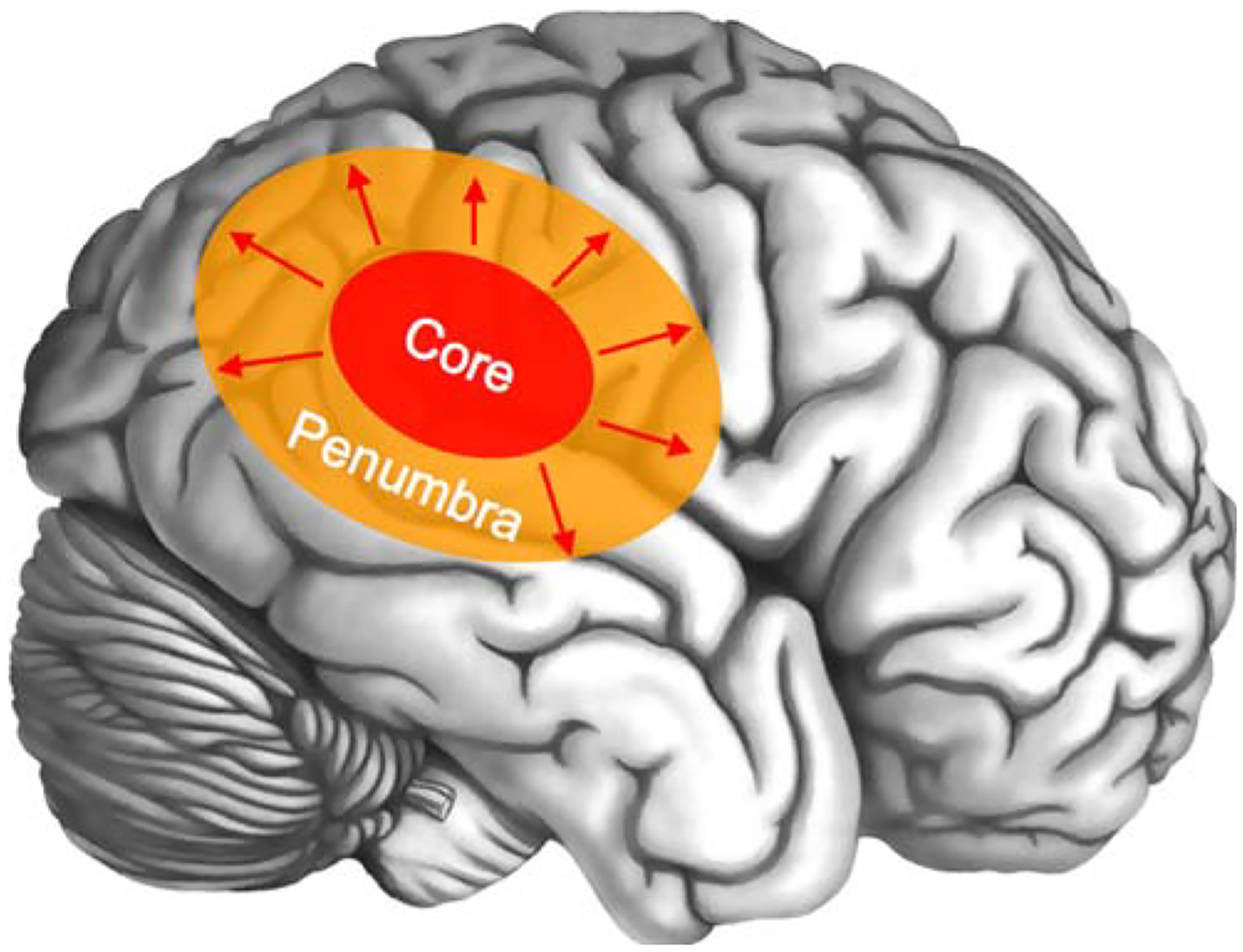
Cerebral stroke is one of the most frequent causes of permanent disability or death in the western world and a major burden in healthcare system. The major portion is caused by acute ischemia due to cerebral artery occlusion by a clot. The minority of strokes is related to intracerebral hemorrhage or other sources. To limit the permanent disability in ischemic stroke patients resulting from irreversible infarction of ischemic brain tissue, major efforts were made in the last decade. To extend the time window for thrombolysis, which is the only approved therapy, several imaging parameters in computed tomography and magnetic resonance imaging (MRI) have been investigated. However, the current guidelines neglect the fact that the portion of potentially salvageable ischemic tissue (penumbra) is not dependent on the time window but the individual collateral blood flow. Within the last years, the differentiation of infarct core and penumbra with MRI using diffusion-weighted images (DWI) and perfusion imaging (PI) with parameter maps was established. Current trials transform these technical advances to a redefined patient selection based on physiological parameters determined by MRI. This review article presents the current status of MRI for acute stroke imaging. A special focus is the ischemic stroke. In dependence on the pathophysiology of cerebral ischemia, the basic principle and diagnostic value of different MRI sequences are illustrated. MRI techniques for imaging of the main differential diagnoses of ischemic stroke are mentioned. Moreover, perspectives of MRI for imaging-based acute stroke treatment as well as monitoring of restorative stroke therapy from recent trials are discussed.
Figures
Comment in
-
Imaging techniques for acute ischemic stroke: nice gadgets or essential tools for effective treatment?Neuroradiology. 2010 Mar;52(3):169-71. doi: 10.1007/s00234-009-0638-0. Epub 2009 Dec 17. Neuroradiology. 2010. PMID: 20016884 No abstract available.
-
Acute stroke imaging.Neuroradiology. 2010 Mar;52(3):173. doi: 10.1007/s00234-009-0639-z. Epub 2010 Jan 22. Neuroradiology. 2010. PMID: 20094708 No abstract available.
References
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G, O’Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y (2009) Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 119:e21–e181 - PubMed
-
- Kolominsky-Rabas PL, Heuschmann PU, Marschall D, Emmert M, Baltzer N, Neundörfer B, Schöffski O, Krobot KJ (2006) Lifetime cost of ischemic stroke in Germany: results and national projections from a population-based stroke registry: the Erlangen Stroke Project. Stroke 37:1179–1183 - PubMed
-
- Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE (1993) Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 24:35–41 - PubMed
-
- Mezzapesa DM, Petruzzellis M, Lucivero V, Prontera M, Tinelli A, Sancilio M, Carella A, Federico F (2006) Multimodal MR examination in acute ischemic stroke. Neuroradiology 48:238–246 - PubMed
-
- Gonzalez RG, Schaefer PW (2006) Conventional MRI and MR angiography of stroke. In: Gonzalez RG, Hirsch JA, Koroshetz WJ, Lev MH, Schaefer P (eds) Acute ischemic stroke: imaging and intervention. Springer, Berlin, pp 115–137
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
