

Factors influencing decisions to admit patients to veterans affairs specialized rehabilitation units after lower-extremity amputation
- PMID: 19969162
- PMCID: PMC2873109
- DOI: 10.1016/j.apmr.2009.07.016
Factors influencing decisions to admit patients to veterans affairs specialized rehabilitation units after lower-extremity amputation
Abstract
Bates BE, Kwong PL, Kurichi JE, Bidelspach DE, Reker DM, Maislin G, Xie D, Stineman M. Factors influencing decisions to admit patients to Veterans Affairs specialized rehabilitation units after lower-extremity amputation.
Objective: To understand patient- and facility-level characteristics that influence decisions to admit veterans to a specialized rehabilitation unit (SRU) after a lower-extremity amputation.
Design: Database study.
Setting: All Veterans Affairs Medical Centers (VAMCs).
Participants: Veterans with lower-extremity amputation discharged from VAMCs between October 1, 2002, and September 30, 2004.
Interventions: Not applicable.
Main outcome measure: Admission to an SRU.
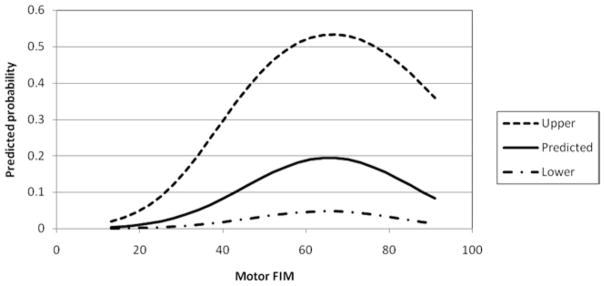
Results: There were a total of 2922 veterans with lower-extremity amputations; 616 patients were admitted to an SRU, whereas 2306 received consultative rehabilitation services only. Patients admitted to an SRU waited longer to have their first rehabilitation assessment after surgery and had middle-range physical and cognitive disabilities. Patients who received consultative rehabilitation services only tended to have greater illness burden. They were more likely to have previous amputation complication, paralysis, or renal failure and either very severe or minimal physical and cognitive disabilities.
Conclusions: The selection of veterans with new lower-extremity amputations for admission to an SRU appears clinically reasonable and based on the likelihood of successful outcomes.
Figures
References
-
- Kaplan SJ. Growth and payment adequacy of medicare postacute care rehabilitation. Arch Phys Med Rehabil. 2007;88:1494–9. - PubMed
-
- Ottenbacher KJ, Graham JE. The state-of-the-science: access to postacute care rehabilitation services. A review Arch Phys Med Rehabil. 2007;88:1513–21. - PubMed
-
- Buntin MB. Access to postacute rehabilitation. Arch Phys Med Rehabil. 2007;88:1488–93. - PubMed
-
- Johnston MV, Graves D, Greene M. The uniform postacute assessment tool: systematically evaluating the quality of measurement evidence. Arch Phys Med Rehabil. 2007;88:1505–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
