

Three synchronous primary carcinomas in a patient with HNPCC associated with a novel germline mutation in MLH1: Case report
- PMID: 19995443
- PMCID: PMC2795749
- DOI: 10.1186/1477-7819-7-94
Three synchronous primary carcinomas in a patient with HNPCC associated with a novel germline mutation in MLH1: Case report
Abstract
Background: MLH1 is one of six known genes responsible for DNA mismatch repair (MMR), whose inactivation leads to HNPCC. It is important to develop genotype-phenotype correlations for HNPCC, as is being done for other hereditary cancer syndromes, in order to guide surveillance and treatment strategies in the future.
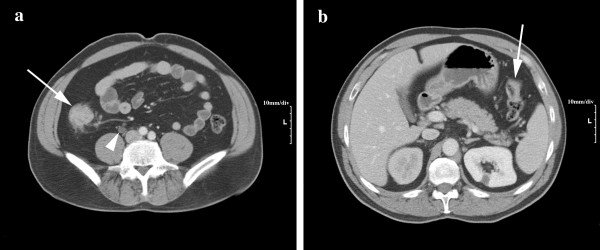
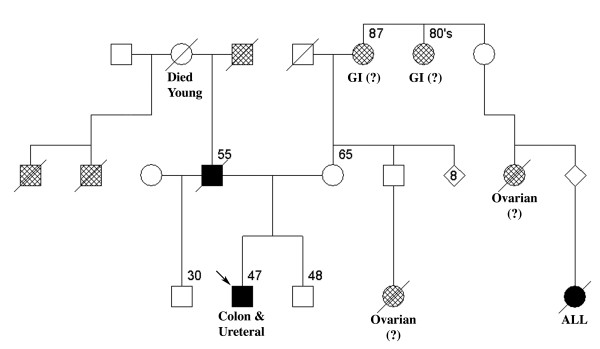
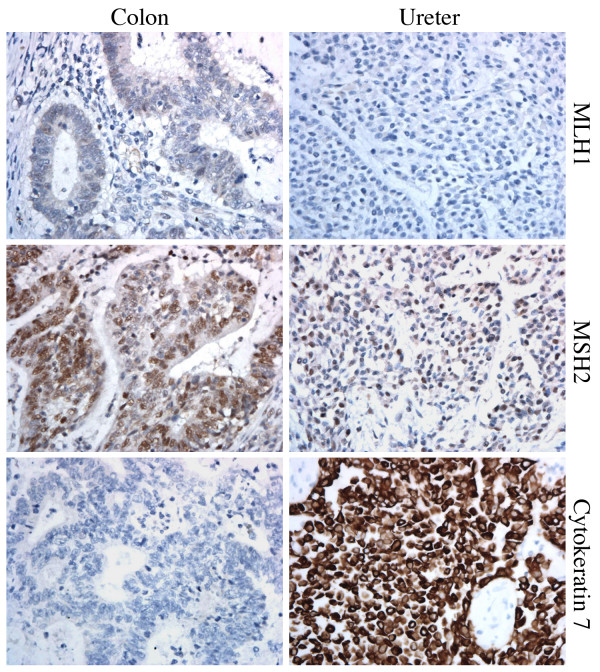
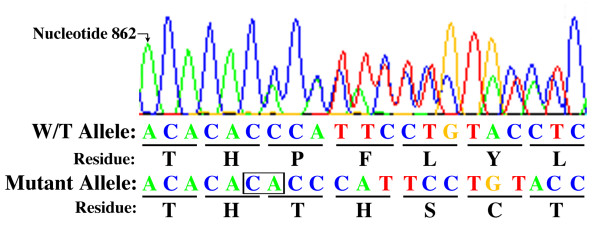
Case presentation: We report a 47 year-old male with hereditary nonpolyposis colorectal cancer (HNPCC) associated with a novel germline mutation in MLH1. This patient expressed a rare and severe phenotype characterized by three synchronous primary carcinomas: ascending and splenic flexure colon adenocarcinomas, and ureteral carcinoma. Ureteral neoplasms in HNPCC are most often associated with mutations in MSH2 and rarely with mutations in MLH1. The reported mutation is a two base pair insertion into exon 10 (c.866_867insCA), which results in a premature stop codon.
Conclusion: Our case demonstrates that HNPCC patients with MLH1 mutations are also at risk for ureteral neoplasms, and therefore urological surveillance is essential. This case adds to the growing list of disease-causing MMR mutations, and contributes to the development of genotype-phenotype correlations essential for assessing individual cancer risk and tailoring of optimal surveillance strategies. Additionally, our case draws attention to limitations of the Amsterdam Criteria and the need to maintain a high index of suspicion when newly diagnosed colorectal cancer meets the Bethesda Criteria. Establishment of the diagnosis is the crucial first step in initiating appropriate surveillance for colorectal cancer and other HNPCC-associated tumors in at-risk individuals.
Figures
Similar articles
-
Association of colonic and endometrial carcinomas in Portuguese families with hereditary nonpolyposis colorectal carcinoma significantly increases the probability of detecting a pathogenic mutation in mismatch repair genes, primarily the MSH2 gene.Cancer. 2004 Jul 1;101(1):172-7. doi: 10.1002/cncr.20320. Cancer. 2004. PMID: 15222003
-
[The first molecular analysis of a Hungarian HNPCC family: a novel MSH2 germline mutation].Orv Hetil. 2005 May 15;146(20):1009-16. Orv Hetil. 2005. PMID: 15945244 Hungarian.
-
MLH1 promoter germline-methylation in selected probands of Chinese hereditary non-polyposis colorectal cancer families.World J Gastroenterol. 2008 Dec 28;14(48):7329-34. doi: 10.3748/wjg.14.7329. World J Gastroenterol. 2008. PMID: 19109866 Free PMC article.
-
Mutations predisposing to hereditary nonpolyposis colorectal cancer.Adv Cancer Res. 1997;71:93-119. doi: 10.1016/s0065-230x(08)60097-4. Adv Cancer Res. 1997. PMID: 9111864 Review.
-
Do MSH6 mutations contribute to double primary cancers of the colorectum and endometrium?Hum Genet. 2000 Dec;107(6):623-9. doi: 10.1007/s004390000417. Hum Genet. 2000. PMID: 11153917 Review.
Cited by
-
Molecular signaling mechanisms of apoptosis in hereditary non-polyposis colorectal cancer.World J Gastrointest Pathophysiol. 2012 Jun 15;3(3):71-9. doi: 10.4291/wjgp.v3.i3.71. World J Gastrointest Pathophysiol. 2012. PMID: 22737591 Free PMC article.
-
Report of a Novel Mutation in MLH1 Gene in a Hispanic Family from Puerto Rico Fulfilling Classic Amsterdam Criteria for Lynch Syndrome.Gastroenterol Res Pract. 2014;2014:527946. doi: 10.1155/2014/527946. Epub 2014 Oct 20. Gastroenterol Res Pract. 2014. PMID: 25389437 Free PMC article.
-
Extracolonic manifestations of lynch syndrome.Clin Colon Rectal Surg. 2012 Jun;25(2):103-10. doi: 10.1055/s-0032-1313781. Clin Colon Rectal Surg. 2012. PMID: 23730225 Free PMC article.
References
-
- Guillem JG, Moore HG. In: ACS Surgery: Principles and Practice. 2006 revised edition. Souba WW, Fink MP, Jurkovich GJ, editor. New York: Web MD Professional Publishing; 2006. Hereditary colorectal cancer and polyposis syndromes; pp. 562–572.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
