

Expectations, validity, and reality in pharmacogenetics
- PMID: 19995676
- PMCID: PMC2888890
- DOI: 10.1016/j.jclinepi.2009.09.006
Expectations, validity, and reality in pharmacogenetics
Abstract
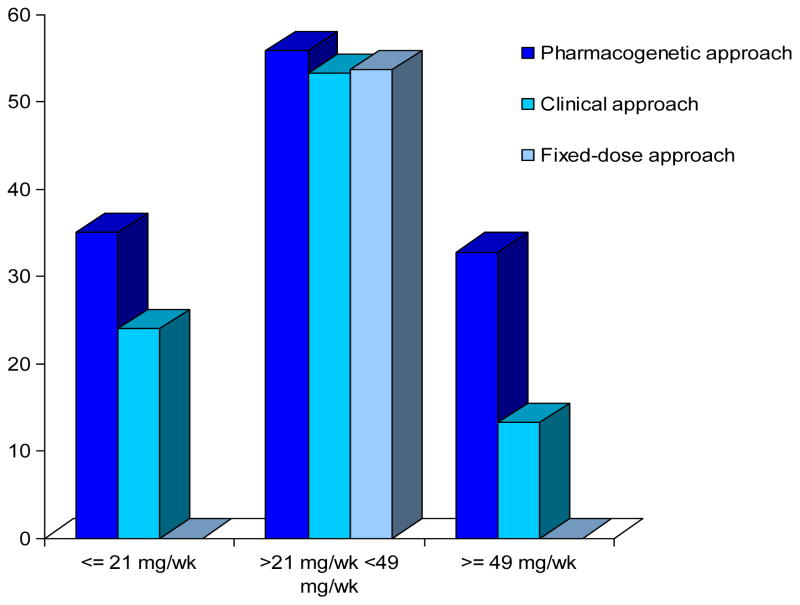
In this review, we discuss the potential expectations, validity, predictive ability, and reality of pharmacogenetics in (1) titration of medication dose, (2) prediction of intended (efficacy) drug response, and (3) dose prediction of unintended (adverse) drug response. We expound on what these potential genetic predictors tell us and, more importantly, what they cannot tell us. Although pharmacogenetic markers have been hailed as promising tools, these proclamations are based mainly on associations rather than their evaluation as predictors. To put the expectations of the promise of pharmacogenetics in a realistic perspective, we review three examples. First, warfarin pharmacogenetics, wherein although the validity of the genetic variant dose is established and there is a validity of genetic variant-hemorrhage association, the clinical utility of testing is not clear. Second, the strong and clinically relevant HLA-Stevens-Johnson syndrome/toxic epidermal necrolysis association highlights the role of ethnicity. Third, the influence of CYP2D6 on tamoxifen efficacy, a model candidate with potential clinical utility but unclear validity. These examples highlight both the challenges and opportunities of pharmacogenomics. First, establishing a valid association between a genetic variation and drug response; second, doing so for a clinically meaningful outcome; and third, providing solid evidence or rationale for improvement in patient outcomes compared with current standard of care.
Figures
Similar articles
-
Pathology consultation on warfarin pharmacogenetic testing.Am J Clin Pathol. 2011 Jan;135(1):13-9. doi: 10.1309/AJCPAO82OTNPUBLW. Am J Clin Pathol. 2011. PMID: 21173120 No abstract available.
-
Tamoxifen pharmacogenomics: the role of CYP2D6 as a predictor of drug response.Clin Pharmacol Ther. 2008 Jan;83(1):160-6. doi: 10.1038/sj.clpt.6100367. Epub 2007 Sep 19. Clin Pharmacol Ther. 2008. PMID: 17882159 Free PMC article. Review.
-
Prediction of tamoxifen outcome by genetic variation of CYP2D6 in post-menopausal women with early breast cancer.Br J Clin Pharmacol. 2014 Apr;77(4):695-703. doi: 10.1111/bcp.12229. Br J Clin Pharmacol. 2014. PMID: 24033728 Free PMC article.
-
Warfarin pharmacogenomics: current best evidence.J Thromb Haemost. 2015 Jun;13 Suppl 1:S266-71. doi: 10.1111/jth.12978. J Thromb Haemost. 2015. PMID: 26149035 Review.
-
The ethics of CYP2D6 testing for patients considering tamoxifen.Breast Cancer Res. 2007;9(2):103. doi: 10.1186/bcr1663. Breast Cancer Res. 2007. PMID: 17433116 Free PMC article.
Cited by
-
Alcohol misuse, genetics, and major bleeding among warfarin therapy patients in a community setting.Pharmacoepidemiol Drug Saf. 2015 Jun;24(6):619-27. doi: 10.1002/pds.3769. Epub 2015 Apr 8. Pharmacoepidemiol Drug Saf. 2015. PMID: 25858232 Free PMC article.
-
Warfarin pharmacogenetics: challenges and opportunities for clinical translation.Front Pharmacol. 2012 Oct 17;3:183. doi: 10.3389/fphar.2012.00183. eCollection 2012. Front Pharmacol. 2012. PMID: 23133417 Free PMC article. No abstract available.
-
Genetic variations in human glutathione transferase enzymes: significance for pharmacology and toxicology.Hum Genomics Proteomics. 2010 Jun 13;2010:876940. doi: 10.4061/2010/876940. Hum Genomics Proteomics. 2010. PMID: 20981235 Free PMC article.
-
The art and science of drug titration.Ther Adv Drug Saf. 2021 Jan 19;11:2042098620958910. doi: 10.1177/2042098620958910. eCollection 2020. Ther Adv Drug Saf. 2021. PMID: 33796256 Free PMC article. Review.
-
Pharmacogenomics in diverse practice settings: implementation beyond major metropolitan areas.Pharmacogenomics. 2015;16(3):227-37. doi: 10.2217/pgs.14.174. Pharmacogenomics. 2015. PMID: 25712186 Free PMC article.
References
-
- Budnitz DS, Shehab N, Kegler SR, Richards CL. Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med. 2007 Dec 4;147(11):755–65. - PubMed
-
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. Jama. 1998 Apr 15;279(15):1200–5. - PubMed
-
- Moore TJ, Cohen MR, Furberg CD. Serious adverse drug events reported to the Food and Drug Administration, 1998–2005. Arch Intern Med. 2007 Sep 10;167(16):1752–9. - PubMed
-
- Ingelman-Sundberg M. Pharmacogenomic biomarkers for prediction of severe adverse drug reactions. N Engl J Med. 2008 Feb 7;358(6):637–9. - PubMed
-
- Manunta P, Bianchi G. Pharmacogenomics and pharmacogenetics of hypertension: update and perspectives--the adducin paradigm. J Am Soc Nephrol. 2006 Apr;17(4 Suppl 2):S30–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
