

Blepharospasm and the modulation of cortical excitability in primary and secondary motor areas
- PMID: 19996078
- PMCID: PMC2790233
- DOI: 10.1212/WNL.0b013e3181c5b42d
Blepharospasm and the modulation of cortical excitability in primary and secondary motor areas
Abstract
Background: Traditionally, benign essential blepharospasm (BEB) is considered a disorder caused by basal ganglia dysfunction. Electrophysiologic and brain imaging studies suggest pathologic changes in excitability in the primary motor cortex (MC), anterior cingulate (AC), and secondary motor areas, such as premotor (PMC) and supplementary motor cortices (SMA).
Methods: In this pilot study of 7 patients with BEB, we experimentally reduced cortical excitability of 4 areas: MC (first dorsal interosseus area), PMC, SMA, and AC, each with 3 noninvasive techniques: low-frequency repetitive transcranial magnetic stimulation (lfrTMS), continuous theta burst stimulation (cTBS), and cathodal transcranial direct current stimulation (tDCS). Primary outcome was the clinical effects on blepharospasm (blink rate observation by an investigator blinded to the intervention and subjective rating by the patient); secondary outcome was the blink reflex recovery curve (BRR).
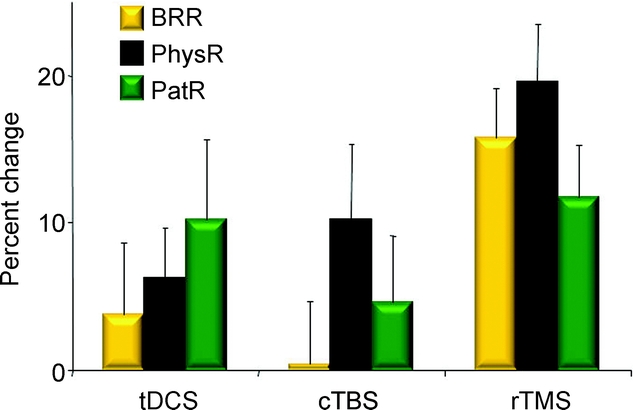
Results: lfrTMS resulted in a significant improvement over all 4 brain areas for physician rating, patient rating, and BRR, whereas cTBS and tDCS showed only trends for improvement in physician rating, but no improvements for patient rating and BRR. lfrTMS had a significantly higher effect over AC than MC for physician rating, but no differences were seen for other pairwise comparisons of stimulated brain areas.
Conclusions: Electrophysiologic and clinical improvements by functional inhibition of the medial frontal areas using low-frequency repetitive transcranial magnetic stimulation suggests that hypersensitivity of the anterior cingulate is directly or indirectly involved in the pathophysiology of benign essential blepharospasm. Inhibition of these areas using low-frequency repetitive transcranial magnetic stimulation could provide a therapeutic tool and is worthy of a larger study.
Figures


References
-
- Müller J, Klemmer G, Wissl J, et al. The impact of blepharospasm and cervical dystonia on health-related quality of life and depression. J Neurol 2002;249:842–684. - PubMed
-
- Hallett M. Dystonia: abnormal movements result from loss of inhibition. In: Fahn S, Hallett M, DeLong M, eds. Advances in Neurology, Volume 94. Philadelphia: Lippincott Williams & Wilkins; 2002:1–7. - PubMed
-
- Curra A, Romaniello A, Berardelli A, et al. Shortened cortical silent period in facial muscles of patients with cranial dystonia. Neurology 2000;54:130–135. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous