

Granulocyte transfusions in severe aplastic anemia: an eleven-year experience
- PMID: 19996117
- PMCID: PMC2791947
- DOI: 10.3324/haematol.2009.010231
Granulocyte transfusions in severe aplastic anemia: an eleven-year experience
Abstract
Background: Infections, particularly those caused by invasive fungi, are a major cause of death in patients with severe aplastic anemia. The purpose of this study was to analyze our experience with granulocyte transfusions in such patients.
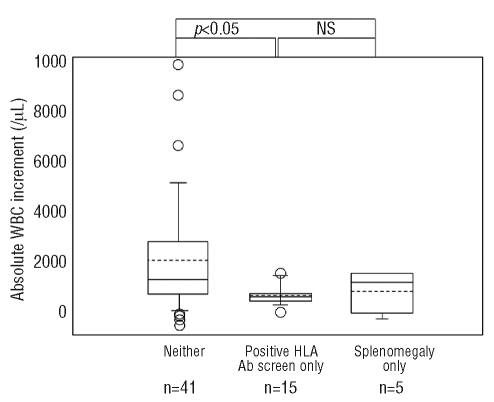
Design and methods: A retrospective analysis was performed on all patients with severe aplastic anemia who had received granulocyte transfusions between 1997 and 2007 in our institute. Survival to hospital discharge was the primary outcome. Secondary outcomes included microbiological, radiographic and clinical responses of the infection at 7 and 30 days after initiating granulocyte therapy, and post-transfusion absolute neutrophil count, stratified by HLA alloimmunization status.
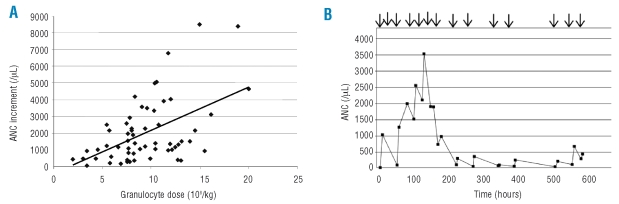
Results: Thirty-two patients with severe aplastic anemia underwent granulocyte transfusions; the majority had received horse antithymocyte globulin and cyclosporine A. One quarter of patients had demonstrable HLA alloimmunization prior to the initiation of granulocyte therapy. Infections were evenly divided between invasive bacterial and fungal infections unresponsive to maximal antibiotic and/or antifungal therapy. The median number of granulocyte components transfused was nine (range, 2-43). The overall survival to hospital discharge was 58%. Survival was strongly correlated with hematopoietic recovery. Among the 18 patients who had invasive fungal infections, 44% survived to hospital discharge. Response at 7 and 30 days correlated with survival. The mean post-transfusion absolute neutrophil count did not differ significantly between response groups (i.e. patients grouped according to whether they had complete or partial resolution of infection, stable disease or progressive infection). There was also no difference in mean post-transfusion absolute neutrophil count between the patients divided according to HLA alloimmunization status.
Conclusions: Granulocyte transfusions may have an adjunctive role in severe infections in patients with severe aplastic anemia. HLA alloimmunization is not an absolute contraindication to granulocyte therapy.
Figures
Comment in
-
Granulocyte transfusion therapy: randomization after all?Haematologica. 2009 Dec;94(12):1644-8. doi: 10.3324/haematol.2009.013680. Haematologica. 2009. PMID: 19996116 Free PMC article.
References
-
- Peters C, Minkov M, Matthes-Martin S, Potschger U, Witt V, Mann G, et al. Leucocyte transfusions from rhG-CSF or prednisolone stimulated donors for treatment of severe infections in immunocompromised neutropenic patients. Br J Haematol. 1999;106:689–96. - PubMed
-
- Price TH, Bowden RA, Boeckh M, Bux J, Nelson K, Liles WC, Dale DC. Phase I/II trial of neutrophil transfusions from donors stimulated with G-CSF and dexamethasone for treatment of patients with infections in hematopoietic stem cell transplantation. Blood. 2000;95:3302–9. - PubMed
-
- Hubel K, Carter RA, Liles WC, Dale DC, Price TH, Bowden RA, et al. Granulocyte transfusion therapy for infections in candidates and recipients of HPC transplantation: a comparative analysis of feasibility and outcome for community donors versus related donors. Transfusion. 2002;42:1414–21. - PubMed
-
- Safdar A, Hanna HA, Boktour M, Kontoyiannis DP, Hachem R, Lichtiger B, et al. Impact of high-dose granulocyte transfusions in patients with cancer with candidemia. Cancer. 2004;101:2859–65. - PubMed
-
- Mousset S, Hermann S, Klein SA, Bialleck H, Duchscherer M, Bomke B, et al. Prophylactic and interventional granulocyte transfusions in patients with haematological malignancies and life-threatening infections during neutropenia. Ann Hematol. 2005;84:734–41. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
