

Differing prevalence and diversity of bacterial species in fetal membranes from very preterm and term labor
- PMID: 19997613
- PMCID: PMC2785424
- DOI: 10.1371/journal.pone.0008205
Differing prevalence and diversity of bacterial species in fetal membranes from very preterm and term labor
Abstract
Background: Intrauterine infection may play a role in preterm delivery due to spontaneous preterm labor (PTL) and preterm prolonged rupture of membranes (PPROM). Because bacteria previously associated with preterm delivery are often difficult to culture, a molecular biology approach was used to identify bacterial DNA in placenta and fetal membranes.
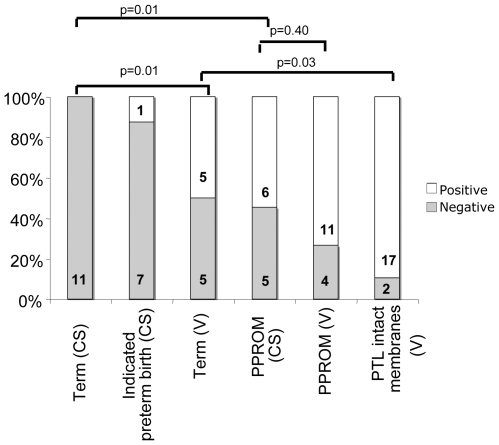
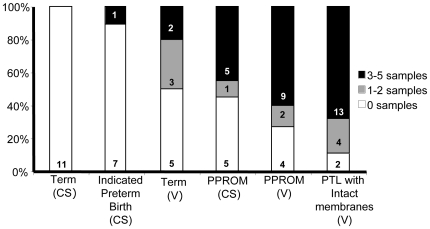
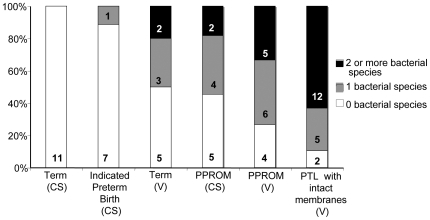
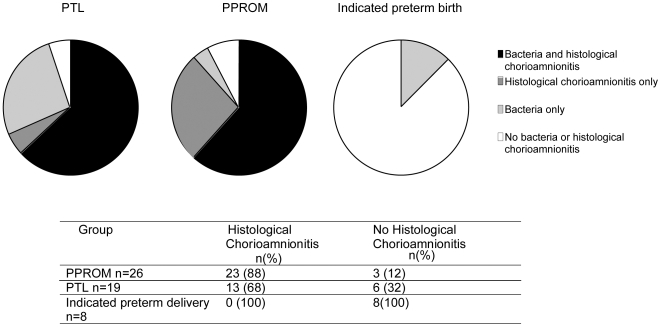
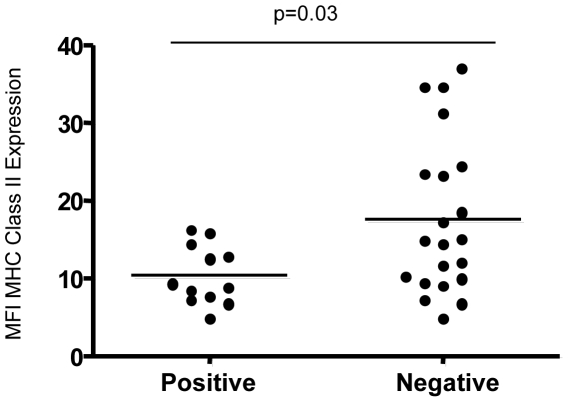
Methodology/principal findings: We used broad-range 16S rDNA PCR and species-specific, real-time assays to amplify bacterial DNA from fetal membranes and placenta. 74 women were recruited to the following groups: PPROM <32 weeks (n = 26; 11 caesarean); PTL with intact membranes <32 weeks (n = 19; all vaginal birth); indicated preterm delivery <32 weeks (n = 8; all caesarean); term (n = 21; 11 caesarean). 50% (5/10) of term vaginal deliveries were positive for bacterial DNA. However, little spread was observed through tissues and species diversity was restricted. Minimal bacteria were detected in term elective section or indicated preterm deliveries. Bacterial prevalence was significantly increased in samples from PTL with intact membranes [89% (17/19) versus 50% (5/10) in term vaginal delivery p = 0.03] and PPROM (CS) [55% (6/11) versus 0% (0/11) in term elective CS, p = 0.01]. In addition, bacterial spread and diversity was greater in the preterm groups with 68% (13/19) PTL group having 3 or more positive samples and over 60% (12/19) showing two or more bacterial species (versus 20% (2/10) in term vaginal deliveries). Blood monocytes from women with PTL with intact membranes and PPROM who were 16S bacterial positive showed greater level of immune paresis (p = 0.03). A positive PCR result was associated with histological chorioamnionitis in preterm deliveries.
Conclusion/significance: Bacteria are found in both preterm and term fetal membranes. A greater spread and diversity of bacterial species were found in tissues of women who had very preterm births. It is unclear to what extent the greater bacterial prevalence observed in all vaginal delivery groups reflects bacterial contamination or colonization of membranes during labor. Bacteria positive preterm tissues are associated with histological chorioamnionitis and a pronounced maternal immune paresis.
Conflict of interest statement
Figures
Similar articles
-
Differential expression pattern of genes encoding for anti-microbial peptides in the fetal membranes of patients with spontaneous preterm labor and intact membranes and those with preterm prelabor rupture of the membranes.J Matern Fetal Neonatal Med. 2009 Dec;22(12):1103-15. doi: 10.3109/14767050902994796. J Matern Fetal Neonatal Med. 2009. PMID: 19916708 Free PMC article.
-
Mitochondrial manganese superoxide dismutase mRNA expression in human chorioamniotic membranes and its association with labor, inflammation, and infection.J Matern Fetal Neonatal Med. 2009 Nov;22(11):1000-13. doi: 10.3109/14767050903019676. J Matern Fetal Neonatal Med. 2009. PMID: 19900038 Free PMC article.
-
Term and preterm labour are associated with distinct microbial community structures in placental membranes which are independent of mode of delivery.Placenta. 2014 Dec;35(12):1099-101. doi: 10.1016/j.placenta.2014.10.007. Epub 2014 Oct 19. Placenta. 2014. PMID: 25458966
-
The role of matrix degrading enzymes and apoptosis in rupture of membranes.J Soc Gynecol Investig. 2004 Oct;11(7):427-37. doi: 10.1016/j.jsgi.2004.04.001. J Soc Gynecol Investig. 2004. PMID: 15458739 Review.
-
Epidemiology and causes of preterm birth.Lancet. 2008 Jan 5;371(9606):75-84. doi: 10.1016/S0140-6736(08)60074-4. Lancet. 2008. PMID: 18177778 Free PMC article. Review.
Cited by
-
Adverse pregnancy and birth outcomes associated with Mycoplasma hominis, Ureaplasma urealyticum and Ureaplasma parvum: a systematic review and meta-analysis.BMJ Open. 2022 Aug 26;12(8):e062990. doi: 10.1136/bmjopen-2022-062990. BMJ Open. 2022. PMID: 36028274 Free PMC article.
-
Toxicant Disruption of Immune Defenses: Potential Implications for Fetal Membranes and Pregnancy.Front Physiol. 2020 May 29;11:565. doi: 10.3389/fphys.2020.00565. eCollection 2020. Front Physiol. 2020. PMID: 32547423 Free PMC article.
-
Protease activities of vaginal Porphyromonas species disrupt coagulation and extracellular matrix in the cervicovaginal niche.NPJ Biofilms Microbiomes. 2022 Feb 21;8(1):8. doi: 10.1038/s41522-022-00270-7. NPJ Biofilms Microbiomes. 2022. PMID: 35190575 Free PMC article.
-
Infant gut microbiota colonization: influence of prenatal and postnatal factors, focusing on diet.Front Microbiol. 2023 Aug 22;14:1236254. doi: 10.3389/fmicb.2023.1236254. eCollection 2023. Front Microbiol. 2023. PMID: 37675422 Free PMC article. Review.
-
Maternal intravenous administration of azithromycin results in significant fetal uptake in a sheep model of second trimester pregnancy.Antimicrob Agents Chemother. 2014 Nov;58(11):6581-91. doi: 10.1128/AAC.03721-14. Epub 2014 Aug 25. Antimicrob Agents Chemother. 2014. PMID: 25155606 Free PMC article.
References
-
- Goldenberg RL, Hauth JC, Andrews WW. Intrauterine infection and preterm delivery. N Eng J Med. 2000;342:1500–1507. - PubMed
-
- Cahill RJ, Dougan G, O'Gaora P, Pickard D, Kennea N, et al. Universal DNA primers amplify bacterial DNA from human fetal membranes and link Fusobacterium nucleatum with prolonged preterm membrane rupture. Mol Hum Reprod. 2005;11:761–765. - PubMed
-
- Kenyon S, Boulvain M, Neilson J. Antibiotics for preterm rupture of membranes. Cochrane Database Syst Rev. 2003;2:CD001058. - PubMed
-
- Hutzal CE, Boyle EM, Kenyon SL, Nash JV, Winsor S, et al. Use of antibiotics for the treatment of preterm parturition and prevention of neonatal morbidity: a metaanalysis. Am J Obstet Gynecol. 2008;199:620.e1–620.e8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
