

SLC26A4 genotype, but not cochlear radiologic structure, is correlated with hearing loss in ears with an enlarged vestibular aqueduct
- PMID: 19998422
- PMCID: PMC2811762
- DOI: 10.1002/lary.20722
SLC26A4 genotype, but not cochlear radiologic structure, is correlated with hearing loss in ears with an enlarged vestibular aqueduct
Abstract
Objectives/hypothesis: Identify correlations among SLC26A4 genotype, cochlear structural anomalies, and hearing loss associated with enlargement of the vestibular aqueduct (EVA).
Study design: Prospective cohort survey, National Institutes of Health, Clinical Center, a federal biomedical research facility.
Methods: Eighty-three individuals, 11 months to 59 years of age, with EVA in at least one ear were studied. Correlations among pure-tone hearing thresholds, number of mutant SLC26A4 alleles, and the presence of cochlear anomalies detected by computed tomography or magnetic resonance imaging were examined.
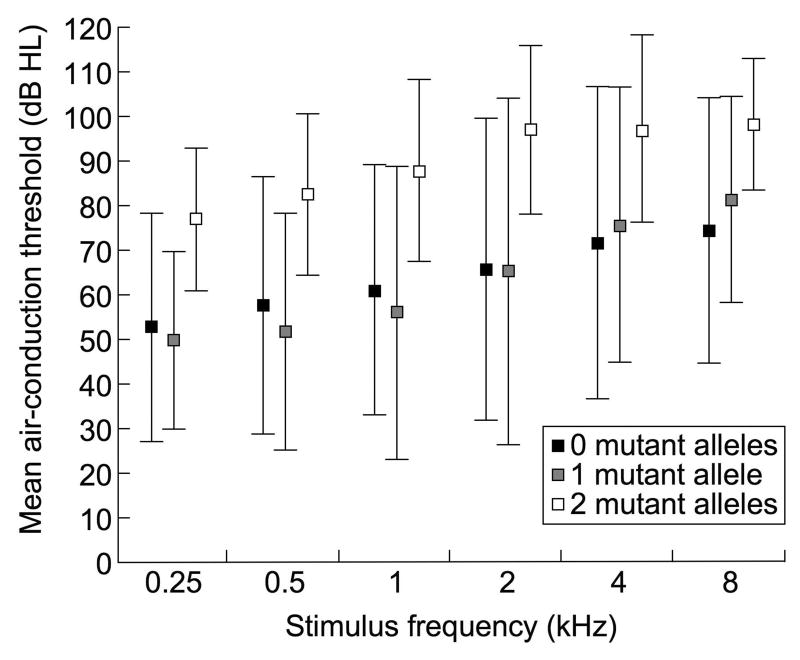
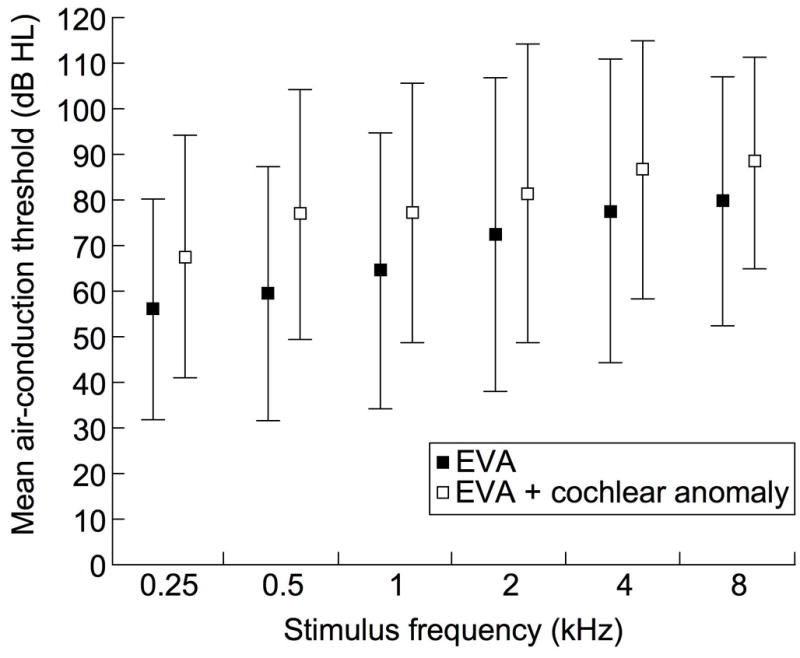
Results: Linear mixed-effects model indicated significantly poorer hearing in ears with EVA in individuals with two mutant alleles of SLC26A4 than in those with EVA and a single mutant allele (P = .012) or no mutant alleles (P = .007) in this gene. There was no detectable relationship between degree of hearing loss and the presence of structural cochlear anomalies.
Conclusions: The number of mutant alleles of SLC26A4, but not the presence of cochlear anomalies, has a significant association with severity of hearing loss in ears with EVA. This information will be useful for prognostic counseling of patients and families with EVA.
Figures
Similar articles
-
Hearing loss associated with enlarged vestibular aqueduct and zero or one mutant allele of SLC26A4.Laryngoscope. 2017 Jul;127(7):E238-E243. doi: 10.1002/lary.26418. Epub 2016 Nov 15. Laryngoscope. 2017. PMID: 27859305 Free PMC article.
-
Atypical patterns of segregation of familial enlargement of the vestibular aqueduct.Laryngoscope. 2016 Jul;126(7):E240-7. doi: 10.1002/lary.25737. Epub 2015 Oct 20. Laryngoscope. 2016. PMID: 26485571 Free PMC article.
-
Subgroups of enlarged vestibular aqueduct in relation to SLC26A4 mutations and hearing loss.Laryngoscope. 2014 Apr;124(4):E134-40. doi: 10.1002/lary.24368. Epub 2013 Dec 17. Laryngoscope. 2014. PMID: 24105851
-
SLC26A4 genotypes and phenotypes associated with enlargement of the vestibular aqueduct.Cell Physiol Biochem. 2011;28(3):545-52. doi: 10.1159/000335119. Epub 2011 Nov 18. Cell Physiol Biochem. 2011. PMID: 22116369 Free PMC article. Review.
-
Genetic architecture and phenotypic landscape of SLC26A4-related hearing loss.Hum Genet. 2022 Apr;141(3-4):455-464. doi: 10.1007/s00439-021-02311-1. Epub 2021 Aug 3. Hum Genet. 2022. PMID: 34345941 Review.
Cited by
-
A common SLC26A4-linked haplotype underlying non-syndromic hearing loss with enlargement of the vestibular aqueduct.J Med Genet. 2017 Oct;54(10):665-673. doi: 10.1136/jmedgenet-2017-104721. Epub 2017 Aug 5. J Med Genet. 2017. PMID: 28780564 Free PMC article.
-
SLC26A4-linked CEVA haplotype correlates with phenotype in patients with enlargement of the vestibular aqueduct.BMC Med Genet. 2019 Jul 2;20(1):118. doi: 10.1186/s12881-019-0853-4. BMC Med Genet. 2019. PMID: 31266487 Free PMC article.
-
Incomplete partition type II in its various manifestations: isolated, in association with EVA, syndromic, and beyond; a multicentre international study.Neuroradiology. 2024 Aug;66(8):1397-1403. doi: 10.1007/s00234-024-03386-z. Epub 2024 Jun 4. Neuroradiology. 2024. PMID: 38833161
-
A novel mutation of TMPRSS3 related to milder auditory phenotype in Korean postlingual deafness: a possible future implication for a personalized auditory rehabilitation.J Mol Med (Berl). 2014 Jun;92(6):651-63. doi: 10.1007/s00109-014-1128-3. Epub 2014 Feb 15. J Mol Med (Berl). 2014. PMID: 24526180
-
SLC26A4 Phenotypic Variability Influences Intra- and Inter-Familial Diagnosis and Management.Genes (Basel). 2022 Nov 23;13(12):2192. doi: 10.3390/genes13122192. Genes (Basel). 2022. PMID: 36553459 Free PMC article.
References
-
- Arcand P, Desrosiers M, Dube J, Abela A. The large vestibular aqueduct syndrome and sensorineural hearing loss in the pediatric population. J Otolaryngol. 1991;20(4):247–250. - PubMed
-
- Okumura T, Takahashi H, Honjo I, Takagi A, Azato R. Magnetic resonance imaging of patients with large vestibular aqueducts. Eur Arch Otorhinolaryngol. 1996;253(7):425–428. - PubMed
-
- Colvin IB, Beale T, Harrop-Griffiths K. Long-term follow-up of hearing loss in children and young adults with enlarged vestibular aqueducts: relationship to radiologic findings and Pendred syndrome diagnosis. Laryngoscope. 2006;116(11):2027–2036. - PubMed
-
- Madden C, Halsted M, Benton C, Greinwald J, Choo D. Enlarged vestibular aqueduct syndrome in the pediatric population. Otol Neurotol. 2003;24(4):625–632. - PubMed
-
- Naganawa S, Koshikawa T, Fukatsu H, et al. Enlarged endolymphatic duct and sac syndrome: relationship between MR findings and genotype of mutation in Pendred syndrome gene. Magn Reson Imaging. 2004;22:25–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
