

Pattern of spread and prognosis in lower limb-onset ALS
- PMID: 20001488
- PMCID: PMC3182546
- DOI: 10.3109/17482960903420140
Pattern of spread and prognosis in lower limb-onset ALS
Abstract
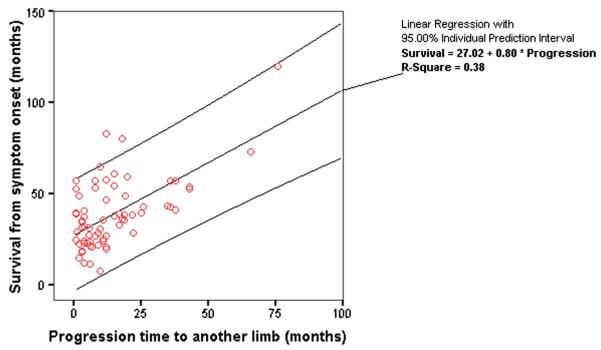
Our objective was to establish the pattern of spread in lower limb-onset ALS (contra- versus ipsi-lateral) and its contribution to prognosis within a multivariate model. Pattern of spread was established in 109 sporadic ALS patients with lower limb-onset, prospectively recorded in Oxford and Sheffield tertiary clinics from 2001 to 2008. Survival analysis was by univariate Kaplan-Meier log-rank and multivariate Cox proportional hazards. Variables studied were time to next limb progression, site of next progression, age at symptom onset, gender, diagnostic latency and use of riluzole. Initial progression was either to the contralateral leg (76%) or ipsilateral arm (24%). Factors independently affecting survival were time to next limb progression, age at symptom onset, and diagnostic latency. Time to progression as a prognostic factor was independent of initial direction of spread. In a regression analysis of the deceased, overall survival from symptom onset approximated to two years plus the time interval for initial spread. In conclusion, rate of progression in lower limb-onset ALS is not influenced by whether initial spread is to the contralateral limb or ipsilateral arm. The time interval to this initial spread is a powerful factor in predicting overall survival, and could be used to facilitate decision-making and effective care planning.
Figures
Similar articles
-
Regional spread pattern predicts survival in patients with sporadic amyotrophic lateral sclerosis.Eur J Neurol. 2012 Jun;19(6):834-41. doi: 10.1111/j.1468-1331.2011.03616.x. Epub 2012 Jan 17. Eur J Neurol. 2012. PMID: 22248150
-
Prognostic value of time to generalization in 71 Chinese patients with sporadic amyotrophic lateral sclerosis.Chin Med J (Engl). 2019 May 5;132(9):1023-1027. doi: 10.1097/CM9.0000000000000200. Chin Med J (Engl). 2019. PMID: 31033570 Free PMC article.
-
Natural history and clinical features of sporadic amyotrophic lateral sclerosis in China.J Neurol Neurosurg Psychiatry. 2015 Oct;86(10):1075-81. doi: 10.1136/jnnp-2015-310471. Epub 2015 Jun 29. J Neurol Neurosurg Psychiatry. 2015. PMID: 26124198
-
Natural history and clinical features of the flail arm and flail leg ALS variants.Neurology. 2009 Mar 24;72(12):1087-94. doi: 10.1212/01.wnl.0000345041.83406.a2. Neurology. 2009. PMID: 19307543 Free PMC article.
-
Amyotrophic Lateral Sclerosis Regional Variants (Brachial Amyotrophic Diplegia, Leg Amyotrophic Diplegia, and Isolated Bulbar Amyotrophic Lateral Sclerosis).Neurol Clin. 2015 Nov;33(4):775-85. doi: 10.1016/j.ncl.2015.07.003. Epub 2015 Sep 8. Neurol Clin. 2015. PMID: 26515621 Free PMC article. Review.
Cited by
-
Clinical and electrophysiological characteristics of respiratory onset amyotrophic lateral sclerosis: a single-centre study.Acta Neurol Belg. 2023 Apr;123(2):391-397. doi: 10.1007/s13760-022-01936-x. Epub 2022 Mar 31. Acta Neurol Belg. 2023. PMID: 35355229
-
Peripheral nerve diffusion tensor imaging as a measure of disease progression in ALS.J Neurol. 2017 May;264(5):882-890. doi: 10.1007/s00415-017-8443-x. Epub 2017 Mar 6. J Neurol. 2017. PMID: 28265751
-
The rostral to caudal gradient of clinical and electrophysiological features in sporadic amyotrophic lateral sclerosis with bulbar-onset.J Int Med Res. 2020 Sep;48(9):300060520956502. doi: 10.1177/0300060520956502. J Int Med Res. 2020. PMID: 32993397 Free PMC article.
-
Different patterns of spreading direction and motor neurons involvement in a cohort of limb-onset amyotrophic lateral sclerosis patients from Southern Italy: Potential implication on disease course or progression?Brain Behav. 2023 Jun;13(6):e2899. doi: 10.1002/brb3.2899. Epub 2023 May 19. Brain Behav. 2023. PMID: 37208847 Free PMC article.
-
Longitudinal course of cortical thickness decline in amyotrophic lateral sclerosis.J Neurol. 2014 Oct;261(10):1871-80. doi: 10.1007/s00415-014-7426-4. Epub 2014 Jul 15. J Neurol. 2014. PMID: 25022938
References
-
- Logroscino G, Traynor BJ, Hardiman O, Chio A, Couratier P, Mitchell JD, et al. Descriptive epidemiology of amyotrophic lateral sclerosis: new evidence and unsolved issues. J Neurol Neurosurg Psychiatry. 2008;79:6–11. - PubMed
-
- Cappellari A, Ciammola A, Silani V. The pseudopolyneuritic form of amyotrophic lateral sclerosis (Patrikios’ disease) Electromyogr Clin Neurophysiol. 2008;48:75–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous