

Regulatory challenges for new drugs to treat obesity and comorbid metabolic disorders
- PMID: 20002080
- PMCID: PMC2810797
- DOI: 10.1111/j.1365-2125.2009.03549.x
Regulatory challenges for new drugs to treat obesity and comorbid metabolic disorders
Abstract
Obesity is a major cause of morbidity and mortality through cardio- and cerebrovascular diseases and cancer. The metabolic consequences of obesity include dyslipidaemia, hypertension, proinflammatory atherogenesis, pre-diabetes and Type 2 diabetes. For a significant proportion of patients, pharmacotherapy to tackle obesity is required as adjunctive support to diet, exercise and lifestyle modification. To this end, the pharmaceutical industry is pursuing many novel drug targets. Although this view is probably not justified, the recent tribulations of rimonabant have created a perception that the regulatory bar for the approval of antiobesity drugs has been raised. Although >5% of placebo-subtracted weight loss maintained over 1 year is the primary efficacy end-point, it is improvements in cardiovascular risk factors that the Food and Drug Administration (FDA) and European Medicines Agency (EMEA) require to grant approval. Safety aspects are also critical in this indication. Many companies are now switching development of their antiobesity drug candidates into other metabolic disorders. Type 2 diabetes is accepted by the industry and FDA, but not EMEA, as the most appropriate alternative. On the other hand, improvements in plasma lipids produced by antiobesity drugs are moderate compared with established therapies, suggesting dyslipidaemia is not a viable development option. Metabolic Syndrome is not accepted by FDA or EMEA as a discrete disease and the agencies will not licence antiobesity drugs for its treatment. The regulatory environment for antiobesity drugs and the spectrum of indications for which they can be approved could change dramatically if positive data for sibutramine emerge from the SCOUT outcome trial.
Figures
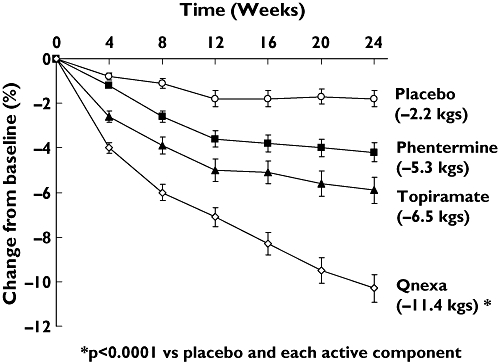
 ); Topiramate (—▴—); Qnexa (—◊—)
); Topiramate (—▴—); Qnexa (—◊—)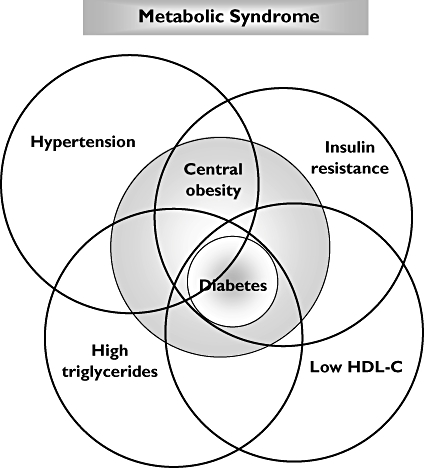
Similar articles
-
[Pharmacological therapy of obesity].G Ital Cardiol (Rome). 2008 Apr;9(4 Suppl 1):83S-93S. G Ital Cardiol (Rome). 2008. PMID: 18773755 Italian.
-
Emerging drugs for obesity: linking novel biological mechanisms to pharmaceutical pipelines.Expert Opin Emerg Drugs. 2005 Aug;10(3):643-60. doi: 10.1517/14728214.10.3.643. Expert Opin Emerg Drugs. 2005. PMID: 16083333 Review.
-
Evolution of pharmacological obesity treatments: focus on adverse side-effect profiles.Diabetes Obes Metab. 2016 Jun;18(6):558-70. doi: 10.1111/dom.12657. Diabetes Obes Metab. 2016. PMID: 26936802 Review.
-
Rise in antiobesity drug prescribing for children and adolescents in the UK: a population-based study.Br J Clin Pharmacol. 2009 Dec;68(6):844-51. doi: 10.1111/j.1365-2125.2009.03528.x. Br J Clin Pharmacol. 2009. PMID: 20002078 Free PMC article.
-
Is there a path for approval of an antiobesity drug: what did the Sibutramine Cardiovascular Outcomes Trial find?Curr Opin Endocrinol Diabetes Obes. 2011 Oct;18(5):321-7. doi: 10.1097/MED.0b013e32834a8726. Curr Opin Endocrinol Diabetes Obes. 2011. PMID: 21878755 Review.
Cited by
-
Developing therapies for the metabolic syndrome: challenges, opportunities, and… the unknown.Ther Adv Endocrinol Metab. 2010 Apr;1(2):89-94. doi: 10.1177/2042018810375812. Ther Adv Endocrinol Metab. 2010. PMID: 23148153 Free PMC article.
-
Rhein Reduces Fat Weight in db/db Mouse and Prevents Diet-Induced Obesity in C57Bl/6 Mouse through the Inhibition of PPARγ Signaling.PPAR Res. 2012;2012:374936. doi: 10.1155/2012/374936. Epub 2012 Sep 25. PPAR Res. 2012. PMID: 23049539 Free PMC article.
-
Pharmacotherapy of obesity: an update on the available medications and drugs under investigation.EClinicalMedicine. 2023 Mar 20;58:101882. doi: 10.1016/j.eclinm.2023.101882. eCollection 2023 Apr. EClinicalMedicine. 2023. PMID: 36992862 Free PMC article. Review.
-
Central and peripheral molecular targets for antiobesity pharmacotherapy.Clin Pharmacol Ther. 2010 Jun;87(6):652-62. doi: 10.1038/clpt.2010.57. Epub 2010 May 5. Clin Pharmacol Ther. 2010. PMID: 20445536 Free PMC article.
-
Acute behavioural effects of bupropion and naltrexone, alone and in combination, in non-deprived male rats presented with palatable mash.Psychopharmacology (Berl). 2013 Jul;228(2):291-307. doi: 10.1007/s00213-013-3036-6. Epub 2013 Mar 1. Psychopharmacology (Berl). 2013. PMID: 23455599
References
-
- International Obesity Task Force (IOTF) Available at http://www.iotf.org (last accessed January 2009.
-
- Daniels SR. The consequences of childhood overweight and obesity. Future Child. 2006;16:47–67. - PubMed
-
- Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. J Am Med Assoc. 2001;286:1195–200. - PubMed
-
- National Cholesterol Education Program. Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) Final report. Circulation. 2002;106:3143–421. - PubMed
-
- Kumanyika S, Jeffery RW, Morabia A, Ritenbaugh C, Antipatis VJ. Obesity prevention: the case for action. Int J Obes. 2002;26:425–36. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
