

Impact of social and economic characteristics on orthodontic treatment among children and teenagers in France
- PMID: 20002629
- PMCID: PMC3085026
- DOI: 10.1111/j.1600-0528.2009.00515.x
Impact of social and economic characteristics on orthodontic treatment among children and teenagers in France
Abstract
Objectives: This study aimed to estimate the prevalence of orthodontic treatment in France among children and teenagers aged 8-18 years, by sex and by age, and to investigate the specific role of social and economic characteristics on use of orthodontic treatment.
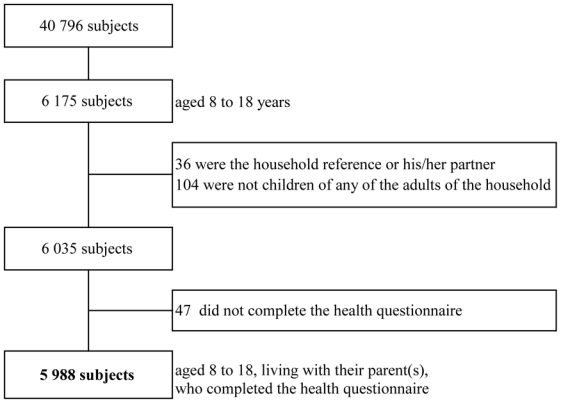
Methods: We analyzed data from the cross-sectional national health survey conducted in France in 2002-2003, which included a sample of 5988 children aged 8-18 years. All data were collected by interview including the question on orthodontic treatment. Other data used in our study were family social status and income, maternal educational attainment and place of birth, whether the child was covered by a supplementary health insurance and whether the residence was urban or rural. We also calculated the density of orthodontists in the district. Multivariate logistic regression analyses were used to study the relationships between these social and economic factors and orthodontic treatment.
Results: The prevalence of orthodontic treatment was 14% of all children aged 8-18, 15% for girls, and 13% for boys, and 23% in the 12 to 15-year age group. Children were less likely to have orthodontic treatment when parents were service or sales workers compared with children whose parents were managers or professionals (aOR = 0.50; 95%CI: [0.34;0.76]), when family income was in the lowest, compared with highest quartile (aOR = 0,62; 95% CI: [0.45;0.85]), when children had no supplementary insurance compared with children covered by private insurance (aOR = 0.53; 95% CI: [0.34; 0.81]), or when they lived in rural compared with urban areas (aOR = 0.70; 95% CI: [0.54; 0.91]).
Conclusion: There are social inequalities in orthodontic treatment in France, associated mainly with social status, annual income, supplementary insurance, and the residence area.
Similar articles
-
Prosthetic treatment in the adult French population: Prevalence and relation with demographic, socioeconomic and medical characteristics.Rev Epidemiol Sante Publique. 2019 Jul;67(4):223-231. doi: 10.1016/j.respe.2019.04.055. Epub 2019 Jun 14. Rev Epidemiol Sante Publique. 2019. PMID: 31204147
-
Epidemiology of malocclusion and orthodontic treatment need of 12-13-year-old Malaysian schoolchildren.Community Dent Health. 2001 Mar;18(1):31-6. Community Dent Health. 2001. PMID: 11421403
-
Socioeconomic determinants of childhood obesity among primary school children in Guangzhou, China.BMC Public Health. 2016 Jun 8;16:482. doi: 10.1186/s12889-016-3171-1. BMC Public Health. 2016. PMID: 27277601 Free PMC article.
-
Disparities in dental insurance coverage and dental care among US children: the National Survey of Children's Health.Pediatrics. 2007 Feb;119 Suppl 1:S12-21. doi: 10.1542/peds.2006-2089D. Pediatrics. 2007. PMID: 17272579
-
Impact of socioeconomic status on children and adolescent's orthodontic treatment; A Systematic Review.Community Dent Health. 2023 May 30;40(2):114-124. doi: 10.1922/CDH_00281Lemasney11. Community Dent Health. 2023. PMID: 37067382
Cited by
-
Socioeconomic burden of orthodontic treatment: a systematic review.Med Pharm Rep. 2023 Apr;96(2):154-163. doi: 10.15386/mpr-2457. Epub 2023 Apr 27. Med Pharm Rep. 2023. PMID: 37197274 Free PMC article. Review.
-
Oral Impacts Experienced by Orthodontic Patients Undergoing Fixed or Removable Appliances Therapy in Saudi Arabia: A Cross-Sectional Study.Patient Prefer Adherence. 2021 Dec 2;15:2683-2691. doi: 10.2147/PPA.S343084. eCollection 2021. Patient Prefer Adherence. 2021. PMID: 34880603 Free PMC article.
-
Equality of specialist orthodontic care for adolescents in the Swedish public dental service: a cohort study.BMC Oral Health. 2025 May 28;25(1):841. doi: 10.1186/s12903-025-06220-x. BMC Oral Health. 2025. PMID: 40437452 Free PMC article.
-
Are Orthodontic Interventions Associated With Headaches in Children and Adolescents? A Systematic Review and Meta-Analysis.Orthod Craniofac Res. 2025 Aug;28(4):656-669. doi: 10.1111/ocr.12911. Epub 2025 Mar 20. Orthod Craniofac Res. 2025. PMID: 40110900 Free PMC article.
-
The impact of an educational pamphlet on the awareness of parents about 4‒6-year-old children's oral habits and dentofacial discrepancies.J Dent Res Dent Clin Dent Prospects. 2016 Winter;10(1):57-64. doi: 10.15171/joddd.2016.009. Epub 2016 Mar 16. J Dent Res Dent Clin Dent Prospects. 2016. PMID: 27092216 Free PMC article.
References
-
- Lathrop ST. The American Heritage Stedman’s Medical Dictionary: Houghton Mifflin. 2005.
-
- Proffit WR, Fields HW, Jr, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13:97–106. - PubMed
-
- Proffit WR. Contemporary orthodontics. 4. St. Louis: Mosby Elsevier; 2007.
-
- ANAES. Recommandations. 2002. Indications de l’orthopédie dento-faciale et dento-maxillo-faciale.
-
- Shaw WC, Addy M, Ray C. Dental and social effects of malocclusion and effectivenessof orthodontic treatment: a review. Community Dent Oral Epidemiol. 1980 Feb;8(1):36–45. - PubMed
