

Mortality after failure of antiretroviral therapy in sub-Saharan Africa
- PMID: 20003034
- PMCID: PMC2873139
- DOI: 10.1111/j.1365-3156.2009.02445.x
Mortality after failure of antiretroviral therapy in sub-Saharan Africa
Abstract
Objective: To assess the outcome of patients who experienced treatment failure with antiretrovirals in sub-Saharan Africa.
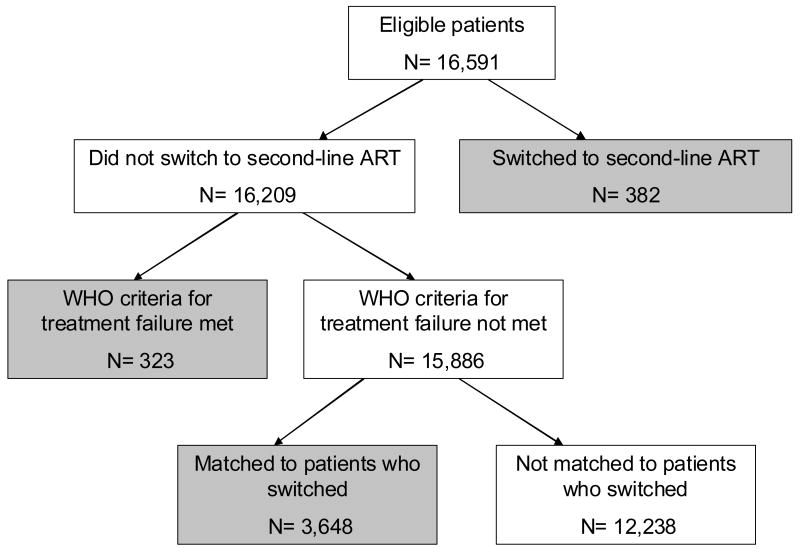
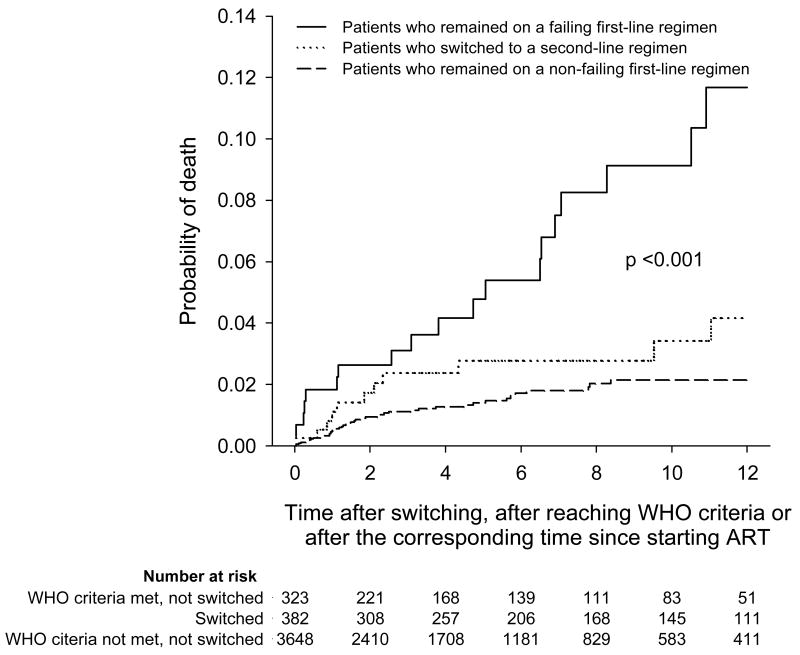
Methods: Analysis of 11 antiretroviral therapy (ART) programmes in sub-Saharan Africa. World Health Organization (WHO) criteria were used to define treatment failure. All ART-naive patients aged >or=16 who started with a non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimen and had at least 6 months of follow-up were eligible. For each patient who switched to a second-line regimen, 10 matched patients who remained on a non-failing first-line regimen were selected. Time was measured from the time of switching, from the corresponding time in matched patients, or from the time of treatment failure in patients who remained on a failing regimen. Mortality was analysed using Kaplan-Meier curves and random-effects Cox models.
Results: Of 16 591 adult patients starting ART, 382 patients (2.3%) switched to a second-line regimen. Another 323 patients (1.9%) did not switch despite developing immunological or virological failure. Cumulative mortality at 1 year was 4.2% (95% CI 2.2-7.8%) in patients who switched to a second-line regimen and 11.7% (7.3%-18.5%) in patients who remained on a failing first-line regimen, compared to 2.2% (1.6-3.0%) in patients on a non-failing first-line regimen (P < 0.0001). Differences in mortality were not explained by nadir CD4 cell count, age or differential loss to follow up.
Conclusions: Many patients who meet criteria for treatment failure do not switch to a second-line regimen and die. There is an urgent need to clarify the reasons why in sub-Saharan Africa many patients remain on failing first-line ART.
Figures
References
-
- Bisson GP, Gross R, Strom JB, et al. Diagnostic accuracy of CD4 cell count increase for virologic response after initiating highly active antiretroviral therapy. AIDS. 2006;20:1613–1619. - PubMed
-
- Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–824. - PubMed
-
- Dabis F, Balestre E, Braitstein P, et al. Antiretroviral Therapy in Lower Income Countries (ART-LINC): International collaboration of treatment cohorts. Int J Epidemiol. 2005;34:979–986. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
