

Gastric cancer surgery: Billroth I or Billroth II for distal gastrectomy?
- PMID: 20003202
- PMCID: PMC2794879
- DOI: 10.1186/1471-2407-9-428
Gastric cancer surgery: Billroth I or Billroth II for distal gastrectomy?
Abstract
Background: The selection of an anastomosis method after a distal gastrectomy is a highly debatable topic; however, the available documentation lacks the necessary research based on a comparison of early postoperative complications. This study was conducted to investigate the difference of early postoperative complications between Billroth I and Billroth II types of anastomosis for distal gastrectomies.
Methods: A total of 809 patients who underwent distal gastrectomies for gastric cancer during four years were included in the study. The only study endpoint was analysis of in-patients' postoperative complications. The risk adjusted complication rate was compared by POSSUM (Physiological and operative severity score for enumeration of morbidity and mortality) and the severity of complications was compared by Rui Jin Hospital classification of complication.
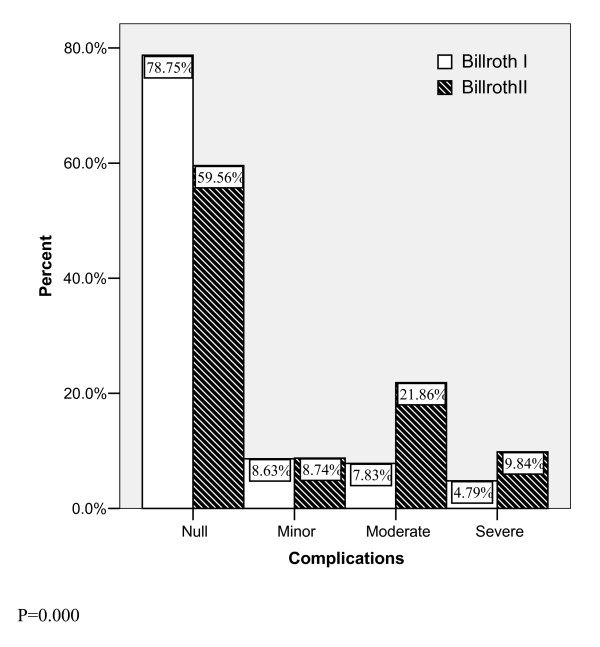
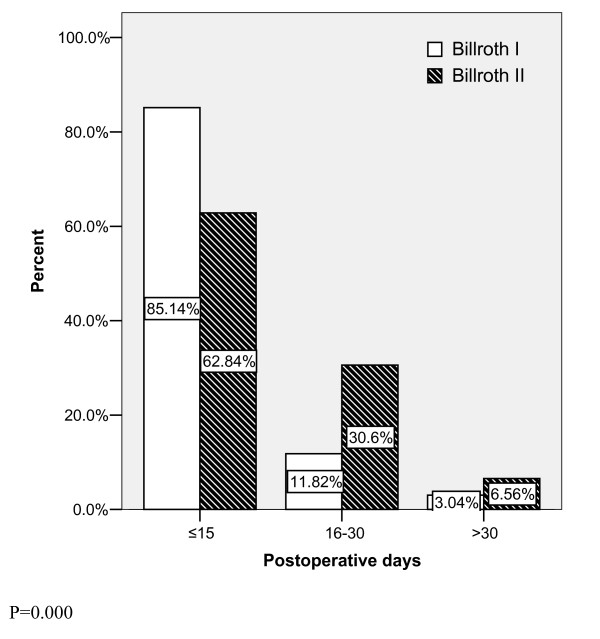
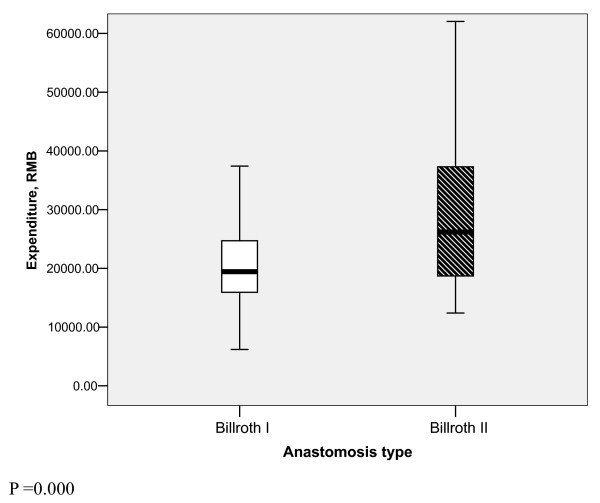
Results: Complication rate of Billroth II type of anastomosis was almost double of that in Billroth I (P=0.000). Similarly, the risk adjusted complication rate was also higher in Billroth II group. More severe complications were observed and the postoperative duration was significantly longer in Billroth II type (P=0.000). Overall expenditure was significantly higher in Billroth II type (P=0.000).
Conclusion: Billroth II method of anastomosis was associated with higher rate of early postoperative complications. Therefore, we conclude that the Billroth I method should be the first choice after a distal gastrectomy as long as the anatomic and oncological environment of an individual patient allows us to perform it. However more prospective studies should be designed to compare the overall surgical outcomes of both anastomosis methods.
Figures
References
-
- Sano T, Sasako M, Yamamoto S, Nashimoto A, Kurita A, Hiratsuka M, Tsujinaka T, Kinoshita T, Arai K, Yamamura Y, Okajima K. Gastric cancer surgery: Morbidity and mortality results from a prospective randomized controlled trial comparing D2 and extended para-aortic lymphadenectomy -- Japan Clinical Oncology Group Study 9501. J Clin Oncol. 2004;22:2767–2773. doi: 10.1200/JCO.2004.10.184. - DOI - PubMed
-
- Roviello F, Marrelli D, Morgagni P, de Manzoni G, Di Leo A, Vindigni C, Saragoni L, Tomezzoli A, Kurihara H. Italian Research Group for Gastric Cancer. Survival benefit of extended D2 lymphadenectomy in gastric cancer with involvement of second level lymph nodes: A longitudinal multicenter study. Ann Surg Oncol. 2002;9:894–900. doi: 10.1007/BF02557527. - DOI - PubMed
-
- Biffi R, Chiappa A, Luca F, Pozzi S, Lo Faso F, Cenciarelli S, Andreoni B. Extended lymph node dissection without routine splenopancreatectomy for treatment of gastric cancer: Low morbidity and mortality rates in a single center series of 250 patients. J Surg Oncol. 2006;93:394–400. doi: 10.1002/jso.20495. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
