

Outcomes following oesophagectomy in patients with oesophageal cancer: a secondary analysis of the ICNARC Case Mix Programme Database
- PMID: 20003248
- PMCID: PMC2791299
- DOI: 10.1186/cc7868
Outcomes following oesophagectomy in patients with oesophageal cancer: a secondary analysis of the ICNARC Case Mix Programme Database
Abstract
Introduction: This report describes the case mix and outcomes of patients with oesophageal cancer admitted to adult critical care units following elective oesophageal surgery in England, Wales and Northern Ireland.
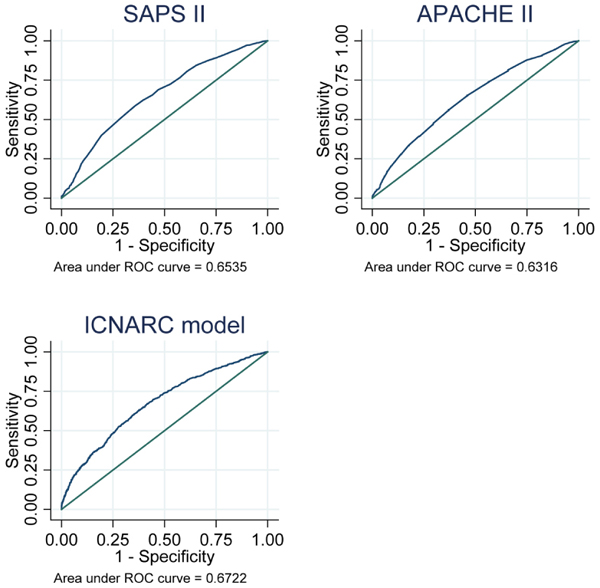
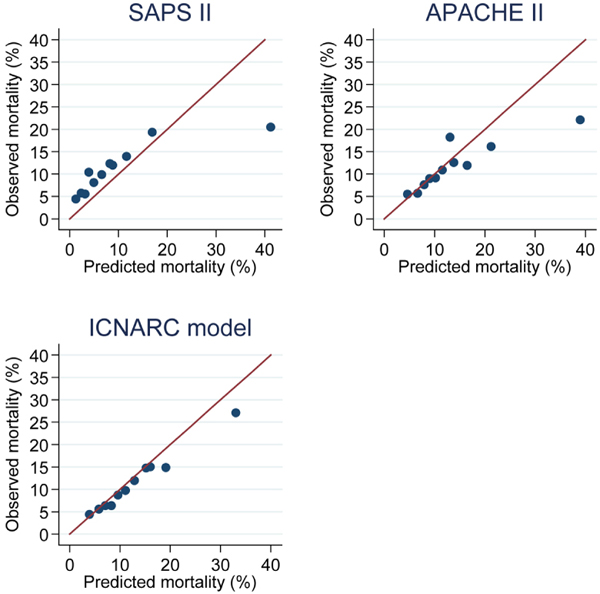
Methods: Admissions to critical care following elective oesophageal surgery for malignancy were identified using data from the Intensive Care National Audit and Research Centre (ICNARC) Case Mix Programme Database. Information on admissions between December 1995 and September 2007 were extracted and the association between in-hospital mortality and patient characteristics on admission to critical care was assessed using multiple logistic regression analysis. The performance of three prognostic models (Simplified Acute Physiology Score (SAPS) II, Acute Physiology and Chronic Health Evaluation (APACHE) II and the ICNARC physiology score) was also evaluated.
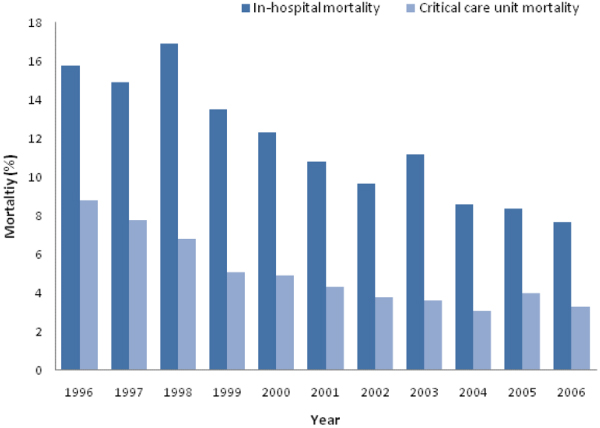
Results: Between 1995 and 2007, there were 7227 admissions to 181 critical care units following oesophageal surgery for malignancy. Overall mortality in critical care was 4.4% and in-hospital mortality was 11%, although both declined steadily over time. Eight hundred and seventy-three (12.2%) patients were readmitted to critical care, most commonly for respiratory complications (49%) and surgical complications (25%). Readmitted patients had a critical care unit mortality of 24.7% and in-hospital mortality of 33.9%. Overall in-hospital mortality was associated with patient age, and various physiological measurements on admission to critical care (partial pressure of arterial oxygen (PaO2):fraction of inspired oxygen (FiO2) ratio, lowest arterial pH, mechanical ventilation, serum albumin, urea and creatinine). The three prognostic models evaluated performed poorly in measures of discrimination, calibration and goodness of fit.
Conclusions: Surgery for oesophageal malignancy continues to be associated with significant morbidity and mortality. Age and organ dysfunction in the early postoperative period are associated with an increased risk of death. Postoperative serum albumin is confirmed as an additional prognostic factor. More work is required to determine how this knowledge may improve clinical management.
Figures
References
-
- National Oesophago-Gastric Cancer Audit: First Annual Report. The NHS Information Centre; 2008.
-
- HESonline: Hospital Episode Statistics. http://www.hesonline.nhs.uk
-
- Lund O, Kimose H, Aagaard M, Hasenkam J, Erlandsen M. Risk stratification and long-term results after surgical treatment of carcinomas of the thoracic esophagus and cardia. A 25-year retrospective study. J Thorac Cardiovasc Surg. 1990;99:200–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
