

A rapid malaria appraisal in the Venezuelan Amazon
- PMID: 20003328
- PMCID: PMC2799431
- DOI: 10.1186/1475-2875-8-291
A rapid malaria appraisal in the Venezuelan Amazon
Abstract
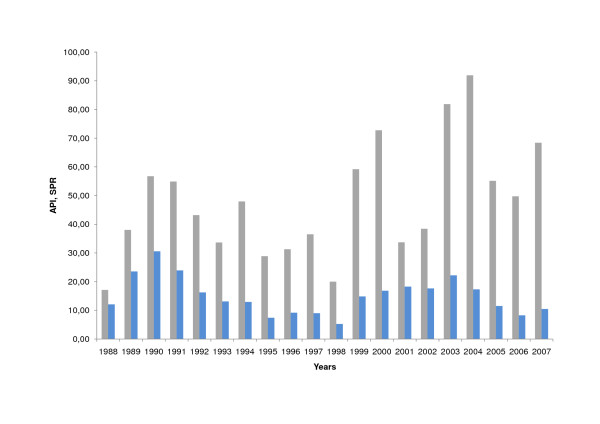
Background: While the federal state of Amazonas bears the highest risk for malaria in Venezuela (2007: 68.4 cases/1000 inhabitants), little comprehensive information about the malaria situation is available from this area. The purpose of this rapid malaria appraisal (RMA) was to provide baseline data about malaria and malaria control in Amazonas.
Methods: The RMA methodology corresponds to a rapid health impact assessment (HIA) as described in the 1999 Gothenburg consensus. In conjunction with the actors of the malaria surveillance system, all useful data and information, which were accessible within a limited time-frame of five visits to Amazonas, were collected, analysed and interpreted.
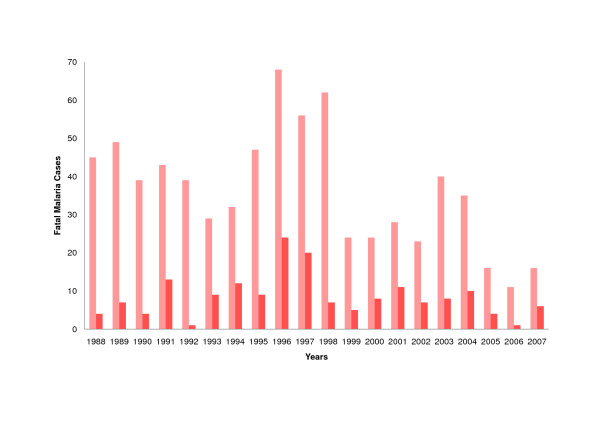
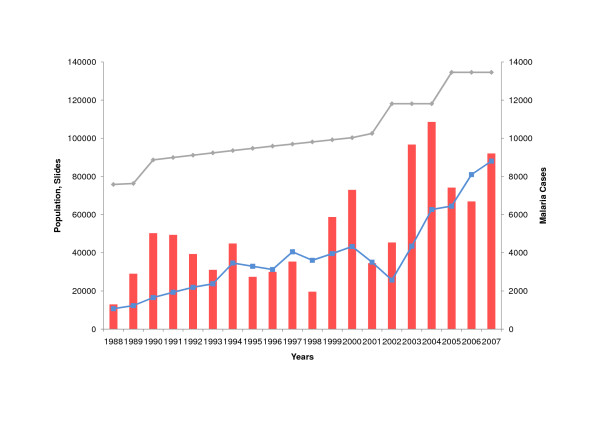
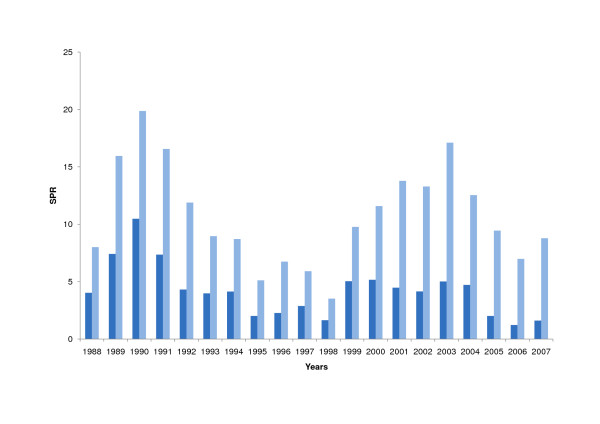
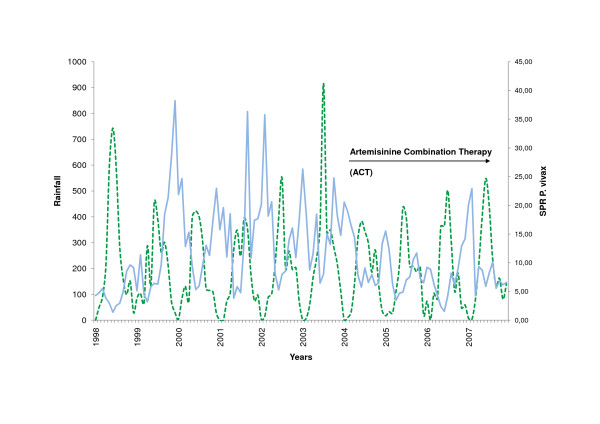
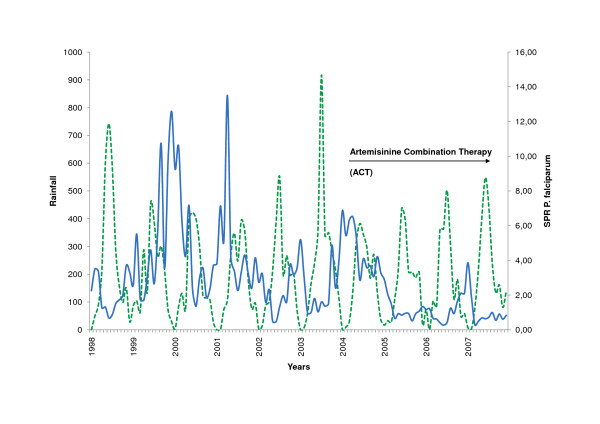
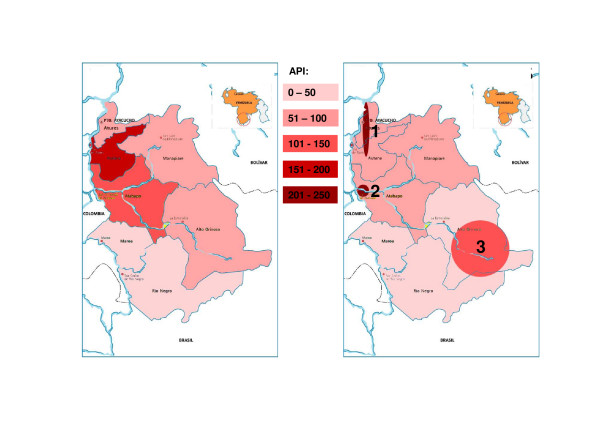
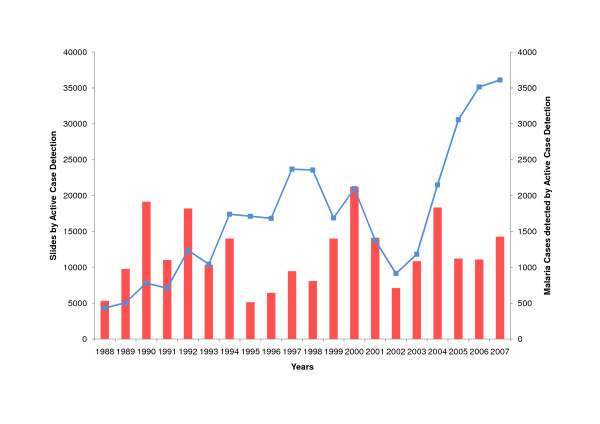
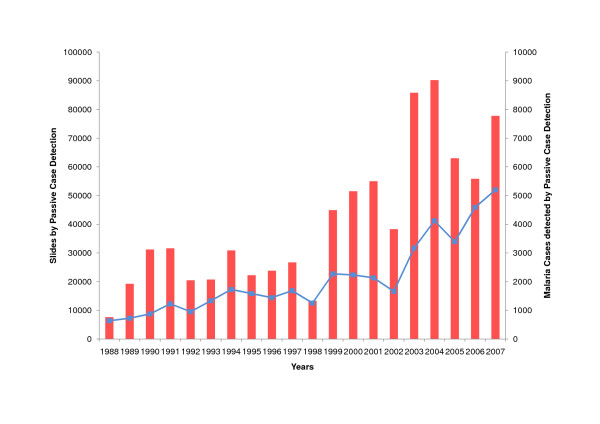
Results: Mortality from malaria is low (< 1 in 105) and slide positivity rates have stayed at the same level for the last two decades (15% +/- 6% (SD)). Active case detection accounts for ca. 40% of slides taken. The coverage of the censured population with malaria notification points (NPs) has been achieved in recent years. The main parasite is Plasmodium vivax (84% of cases). The proportion of Plasmodium falciparum is on the decline, possibly driven by the introduction of cost-free artemisinin-based combination therapy (ACT) (1988: 33.4%; 2007: 15.4%). Monitoring and documentation is complete, systematic and consistent, but poorly digitalized. Malaria transmission displayed a visible lag behind rainfall in the capital municipality of Atures, but not in the other municipalities. In comparison to reference microscopy, quality of field microscopy and rapid diagnostic tests (RDTs) is suboptimal (kappa < 0.75). Hot spots of malaria risk were seen in some indigenous ethnic groups. Conflicting strategies in respect of training of community health workers (CHW) and the introduction of new diagnostic tools (RDTs) were observed.
Conclusion: Malaria control is possible, even in tropical rain forest areas, if the health system is working adequately. Interventions have to be carefully designed and the features of the particular local Latin American context considered.
Figures
References
-
- Alais ML. La población indígena de Venezuela según los censos nacionales. Encuentro nacional de demógrafos y estudiosos de la población. 2004.
-
- Gabaldon A, Berti L. The First large area in the tropical zone to report malaria eradication: north-central Venezuela. Am J Trop Med Hyg. 1954;3:793–807. - PubMed
-
- Sanchez E, Perez HA, Martinez C. Malaria in the Amazon. Prevalence of Plasmodium falciparum antibodies in Amerindians inhabiting the Venezuelan Amazon. Ann Trop Med Parasitol. 1990;84:307–312. - PubMed
-
- Perez MS. Anemia and malaria in a Yanomami Amerindian population from the southern Venezuelan Amazon. Am J Trop Med Hyg. 1998;59:998–1001. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
