

Visualization of anomalous origin and course of coronary arteries in 748 consecutive symptomatic patients by 64-slice computed tomography angiography
- PMID: 20003347
- PMCID: PMC2799381
- DOI: 10.1186/1471-2261-9-54
Visualization of anomalous origin and course of coronary arteries in 748 consecutive symptomatic patients by 64-slice computed tomography angiography
Abstract
Background: Coronary artery anomalies (CAAs) are currently undergoing profound changes in understanding potentially pathophysiological mechanisms of disease. Aim of this study was to investigate the prevalence of anomalous origin and course of coronary arteries in consecutive symptomatic patients, who underwent cardiac 64-slice multidetector-row computed tomography angiography (MDCTA).
Methods: Imaging datasets of 748 consecutive symptomatic patients referred for cardiac MDCTA were analyzed and CAAs of origin and further vessel course were grouped according to a recently suggested classification scheme by Angelini et al.
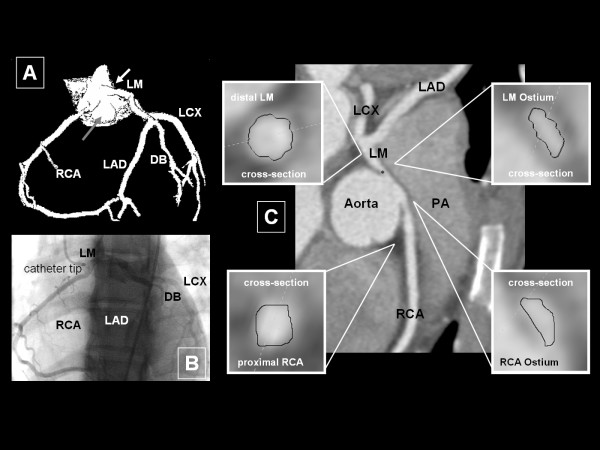
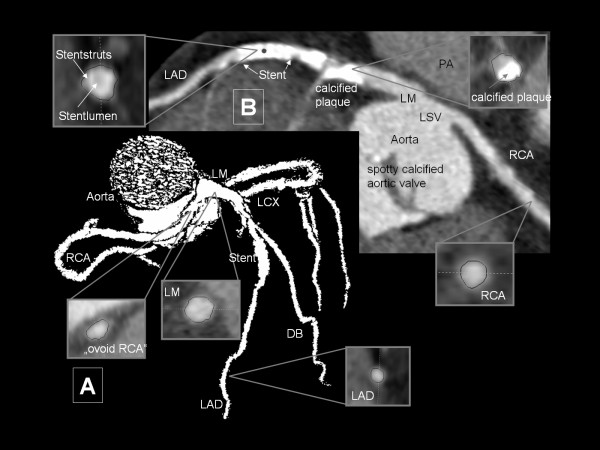
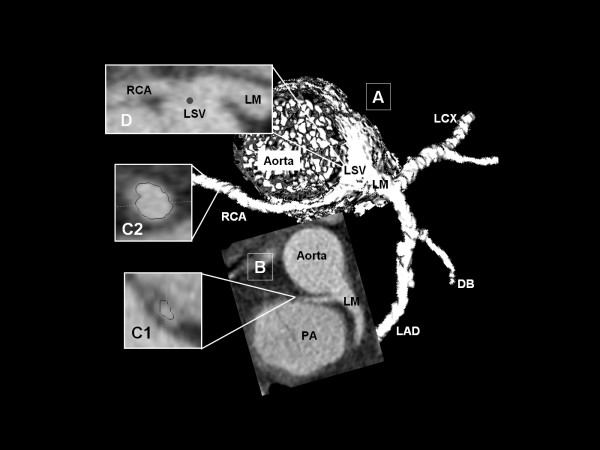
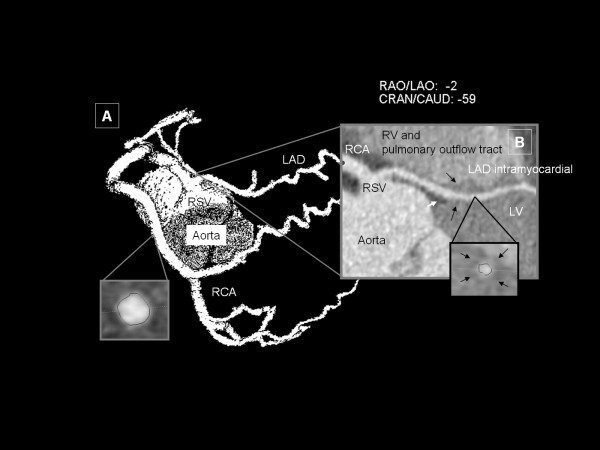
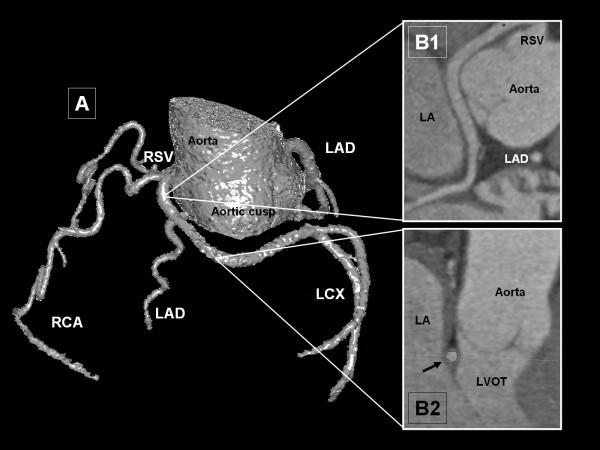
Results: An overall of 17/748 patients (2.3%) showed CAA of origin and further vessel course. According to aforementioned classification scheme no Subgroup 1- (absent left main trunk) and Subgroup 2- (anomalous location of coronary ostium within aortic root or near proper aortic sinus of Valsalva) CAA were found. Subgroup 3 (anomalous location of coronary ostium outside normal "coronary" aortic sinuses) consisted of one patient with high anterior origin of both coronary arteries. The remaining 16 patients showed a coronary ostium at improper sinus (Subgroup 4). Latter group was subdivided into a right coronary artery arising from left anterior sinus with separate ostium (subgroup 4a; n = 7) and common ostium with left main coronary artery (subgroup 4b; n = 1). Subgroup 4c consisted of one patient with a single coronary artery arising from the right anterior sinus (RAS) without left circumflex coronary artery (LCX). In subgroup 4d, LCX arose from RAS (n = 7).
Conclusions: Prevalence of CAA of origin and further vessel course in a symptomatic consecutive patient population was similar to large angiographic series, although these patients do not reflect general population. However, our study supports the use of 64-slice MDCTA for the identification and definition of CAA.
Figures
Similar articles
-
Prevalence and characteristics of coronary artery anomalies in an adult population undergoing multidetector-row computed tomography for the evaluation of coronary artery disease.BMC Cardiovasc Disord. 2015 Oct 2;15:112. doi: 10.1186/s12872-015-0098-x. BMC Cardiovasc Disord. 2015. PMID: 26431696 Free PMC article.
-
Prevalence and characteristics of coronary anomalies originating from the opposite sinus of Valsalva in 8,522 patients referred for coronary computed tomography angiography.Am J Cardiol. 2013 May 1;111(9):1361-7. doi: 10.1016/j.amjcard.2013.01.280. Epub 2013 Feb 11. Am J Cardiol. 2013. PMID: 23411107
-
Coronary arteries anomalous aortic origin on a computed tomography angiography population: prevalence, characteristics and clinical impact.Int J Cardiovasc Imaging. 2016 Jun;32(6):983-90. doi: 10.1007/s10554-016-0849-5. Epub 2016 Feb 6. Int J Cardiovasc Imaging. 2016. PMID: 26852241
-
Frequency in the anomalous origin of the right coronary artery with angiography in a Turkish population.Int J Cardiol. 2002 Mar;82(3):253-7. doi: 10.1016/s0167-5273(02)00002-5. Int J Cardiol. 2002. PMID: 11911913 Review.
-
A rare coronary anomaly consisting of a single right coronary ostium in an adult undergoing surgical coronary revascularization: a case report and review of the literature.J Med Case Rep. 2016 Jul 1;10(1):190. doi: 10.1186/s13256-016-0977-5. J Med Case Rep. 2016. PMID: 27370010 Free PMC article. Review.
Cited by
-
Anomalous aortic origin of coronary arteries from the opposite sinus: a critical appraisal of risk.BMC Cardiovasc Disord. 2012 Oct 1;12:83. doi: 10.1186/1471-2261-12-83. BMC Cardiovasc Disord. 2012. PMID: 23025810 Free PMC article. Review.
-
Anomalous origination of a coronary artery from the opposite sinus.Nat Rev Cardiol. 2011 Oct 11;8(12):706-19. doi: 10.1038/nrcardio.2011.147. Nat Rev Cardiol. 2011. PMID: 21989050 Review.
-
Anatomical variants and coronary anomalies detected by dual-source coronary computed tomography angiography in North-eastern Thailand.Pol J Radiol. 2018 Sep 17;83:e372-e378. doi: 10.5114/pjr.2018.78420. eCollection 2018. Pol J Radiol. 2018. PMID: 30655913 Free PMC article.
-
Anomalous right coronary artery in a middle-aged patient: A case report and review of the literature.Medicine (Baltimore). 2016 Dec;95(49):e5508. doi: 10.1097/MD.0000000000005508. Medicine (Baltimore). 2016. PMID: 27930539 Free PMC article.
-
Prevalence and characteristics of coronary artery anomalies (CAAS) in 3016 symptomatic adult participants undergoing coronary computed tomography angiography (CCTA): A single-center retrospective study in Iran.J Cardiovasc Thorac Res. 2023;15(4):218-222. doi: 10.34172/jcvtr.2023.32860. Epub 2023 Dec 30. J Cardiovasc Thorac Res. 2023. PMID: 38357563 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
