

Monte Carlo vs. pencil beam based optimization of stereotactic lung IMRT
- PMID: 20003380
- PMCID: PMC2801495
- DOI: 10.1186/1748-717X-4-64
Monte Carlo vs. pencil beam based optimization of stereotactic lung IMRT
Abstract
Background: The purpose of the present study is to compare finite size pencil beam (fsPB) and Monte Carlo (MC) based optimization of lung intensity-modulated stereotactic radiotherapy (lung IMSRT).
Materials and methods: A fsPB and a MC algorithm as implemented in a biological IMRT planning system were validated by film measurements in a static lung phantom. Then, they were applied for static lung IMSRT planning based on three different geometrical patient models (one phase static CT, density overwrite one phase static CT, average CT) of the same patient. Both 6 and 15 MV beam energies were used. The resulting treatment plans were compared by how well they fulfilled the prescribed optimization constraints both for the dose distributions calculated on the static patient models and for the accumulated dose, recalculated with MC on each of 8 CTs of a 4DCT set.
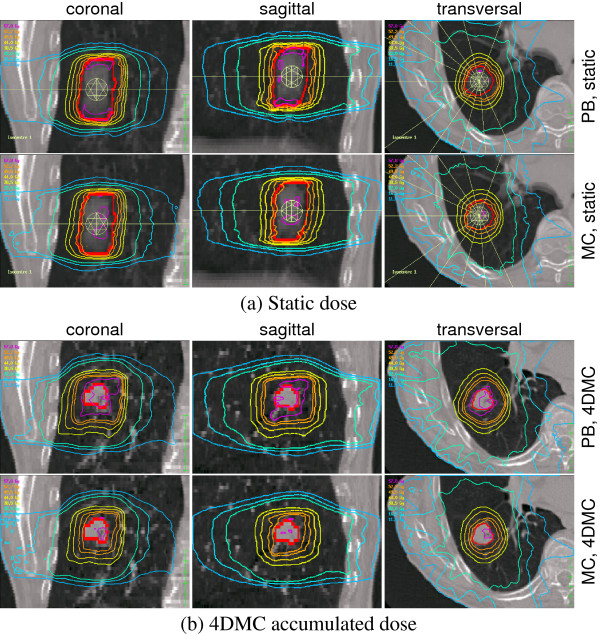
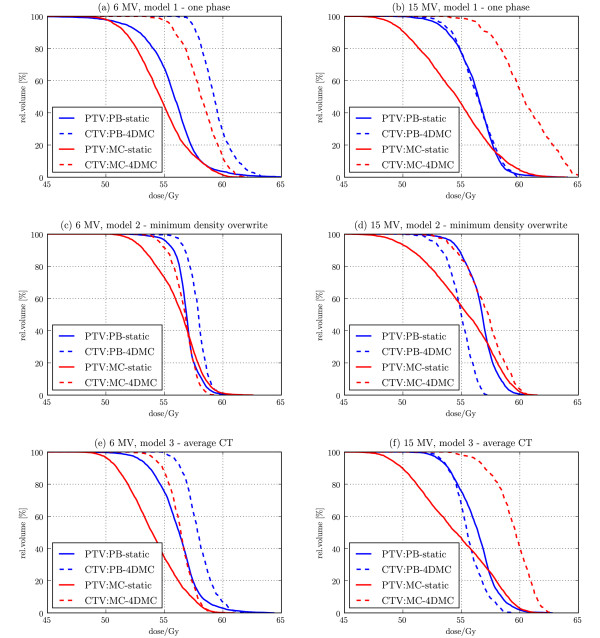
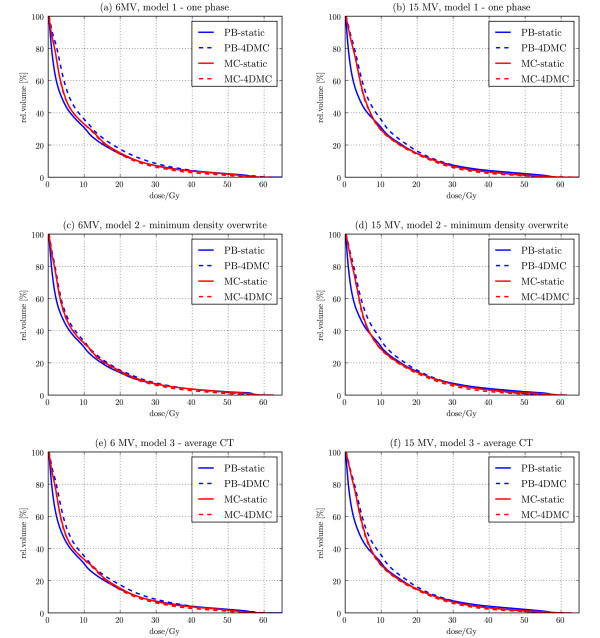
Results: In the phantom measurements, the MC dose engine showed discrepancies < 2%, while the fsPB dose engine showed discrepancies of up to 8% in the presence of lateral electron disequilibrium in the target. In the patient plan optimization, this translates into violations of organ at risk constraints and unpredictable target doses for the fsPB optimized plans. For the 4D MC recalculated dose distribution, MC optimized plans always underestimate the target doses, but the organ at risk doses were comparable. The results depend on the static patient model, and the smallest discrepancy was found for the MC optimized plan on the density overwrite one phase static CT model.
Conclusions: It is feasible to employ the MC dose engine for optimization of lung IMSRT and the plans are superior to fsPB. Use of static patient models introduces a bias in the MC dose distribution compared to the 4D MC recalculated dose, but this bias is predictable and therefore MC based optimization on static patient models is considered safe.
Figures
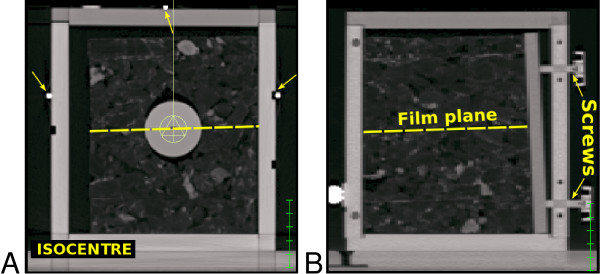
 with an average density of ρmean = 0.12 , while the plastic sphere had a density of ρ = 1.1 . A film could be positioned through the phantom as marked with a dashed line in A and B. The cork cube, plastic sphere and film were fixed relatively to the high density positioning markers (indicated by arrows on A) on the surface of the plastic container by a plastic plate and four plastic screws as shown in B.
with an average density of ρmean = 0.12 , while the plastic sphere had a density of ρ = 1.1 . A film could be positioned through the phantom as marked with a dashed line in A and B. The cork cube, plastic sphere and film were fixed relatively to the high density positioning markers (indicated by arrows on A) on the surface of the plastic container by a plastic plate and four plastic screws as shown in B.
References
-
- Paelinck L, Reynaert N, Thierens H, De Neve W, De Wagter C. Experimental verification of lung dose with radiochromic film: comparison with Monte Carlo simulations and commercially available treatment planning systems. Phys Med Biol. 2005;50(9):2055–69. doi: 10.1088/0031-9155/50/9/009. - DOI - PubMed
-
- Solberg TD, Holly FE, De Salles AA, Wallace RE, Smathers JB. Implications of tissue heterogeneity for radiosurgery in head and neck tumors. Int J Radiat Oncol Biol Phys. 1995;32:235–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
