

Universal health care no guarantee of equity: comparison of socioeconomic inequalities in the receipt of coronary procedures in patients with acute myocardial infarction and angina
- PMID: 20003401
- PMCID: PMC2807435
- DOI: 10.1186/1471-2458-9-460
Universal health care no guarantee of equity: comparison of socioeconomic inequalities in the receipt of coronary procedures in patients with acute myocardial infarction and angina
Abstract
Background: In Australia there is a socioeconomic gradient in morbidity and mortality favouring socioeconomically advantaged people, much of which is accounted for by ischaemic heart disease. This study examines if Australia's universal health care system, with its mixed public/private funding and delivery model, may actually perpetuate this inequity. We do this by quantifying and comparing socioeconomic inequalities in the receipt of coronary procedures in patients with acute myocardial infarction (AMI) and patients with angina.
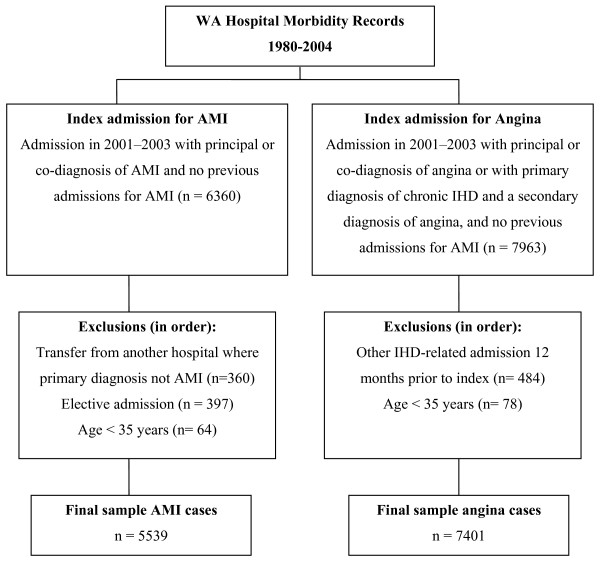
Methods: Using linked hospital and mortality data, we followed patients admitted to Western Australian hospitals with a first admission for AMI (n = 5539) or angina (n = 7401) in 2001-2003. An outcome event was the receipt, within a year, of a coronary procedure-angiography, angioplasty and/or coronary artery bypass surgery (CABG). Socioeconomic status was assigned to each individual using an area-based measure, the SEIFA Index of Disadvantage. Multivariable proportional hazards regression was used to model the association between socioeconomic status and procedure rates, allowing for censoring and adjustment of multiple covariates. Mediating models examined the effect of private health insurance.
Results: In the AMI patient cohort, socioeconomic gradients were not evident except that disadvantaged women were more likely than advantaged women to undergo CABG. In contrast, in the angina patient group there were clear socioeconomic gradients for all procedures, favouring more advantaged patients. Compared with patients in the most disadvantaged quintile of socioeconomic status, patients in the least disadvantaged quintile were 11% (1-21%) more likely to receive angiography, 52% (29-80%) more likely to undergo angioplasty and 30% (3-55%) more likely to undergo CABG. Private health insurance explained some of the socioeconomic variation in rates.
Conclusions: Australia's universal health care system does not guarantee equity in the receipt of high technology health care for patients with ischaemic heart disease. While such a system might ensure equity for patients with AMI, where guidelines for treatment are relatively well established, this is not the case for angina patients, where health care may be less urgent and more discretionary.
Similar articles
-
Education-related variation in coronary procedure rates and the contribution of private health care in Australia: a prospective cohort study.Int J Equity Health. 2020 Aug 14;19(1):139. doi: 10.1186/s12939-020-01235-y. Int J Equity Health. 2020. PMID: 32795313 Free PMC article.
-
Variation in cardiovascular disease care: an Australian cohort study on sex differences in receipt of coronary procedures.BMJ Open. 2019 Jul 23;9(7):e026507. doi: 10.1136/bmjopen-2018-026507. BMJ Open. 2019. PMID: 31337660 Free PMC article.
-
Socioeconomic inequalities in the diffusion of health technology: Uptake of coronary procedures as an example.Soc Sci Med. 2011 Jan;72(2):224-9. doi: 10.1016/j.socscimed.2010.11.002. Epub 2010 Nov 23. Soc Sci Med. 2011. PMID: 21147510
-
Sex differences in the use of invasive coronary procedures in Ontario.Can J Cardiol. 1994 Mar;10(2):239-44. Can J Cardiol. 1994. PMID: 8143225 Review.
-
Management of chronic stable angina: medical therapy, percutaneous transluminal coronary angioplasty, and coronary artery bypass graft surgery. Lessons from the randomized trials.Ann Intern Med. 1998 Feb 1;128(3):216-23. doi: 10.7326/0003-4819-128-3-199802010-00008. Ann Intern Med. 1998. PMID: 9454530 Review.
Cited by
-
Outcomes after first percutaneous coronary intervention for acute myocardial infarction according to patient funding source.BMC Health Serv Res. 2014 Sep 18;14:405. doi: 10.1186/1472-6963-14-405. BMC Health Serv Res. 2014. PMID: 25231072 Free PMC article.
-
Cardiac procedures in ST-segment-elevation myocardial infarction - the influence of age, geography and Aboriginality.BMC Cardiovasc Disord. 2020 May 14;20(1):224. doi: 10.1186/s12872-020-01487-0. BMC Cardiovasc Disord. 2020. PMID: 32408860 Free PMC article.
-
The effect of extension of benefit coverage for cancer patients on health care utilization across different income groups in South Korea.Int J Health Care Finance Econ. 2014 Jun;14(2):161-77. doi: 10.1007/s10754-014-9144-y. Epub 2014 Apr 2. Int J Health Care Finance Econ. 2014. PMID: 24691773
-
Inequalities in ventilation tube insertion procedures between Aboriginal and non-Aboriginal children in New South Wales, Australia: a data linkage study.BMJ Open. 2013 Nov 27;3(11):e003807. doi: 10.1136/bmjopen-2013-003807. BMJ Open. 2013. PMID: 24285631 Free PMC article.
-
The impact of population-based disease management services for selected chronic conditions: the Costs to Australian Private Insurance--Coaching Health (CAPICHe) study protocol.BMC Public Health. 2012 Feb 10;12:114. doi: 10.1186/1471-2458-12-114. BMC Public Health. 2012. PMID: 22325668 Free PMC article. Clinical Trial.
References
-
- Draper G, Turrell G, Oldenburg B. Health inequalities in Australia: mortality. Health inequalities monitoring series No. 1. AIHW cat. no. PHE 55. Brisbane and Canberra: Queensland University of Technology and the Australian Institute of Health and Welfare; 2004.
-
- Page A, Tobias M, Glover J, Wright C, Hertzel D, Fisher E. Australian and New Zealand atlas of avoidable mortality. Adelaide: PHIDU, University of Adelaide; 2006.
-
- Pincus T, Esther R, DeWalt DA, Callahan LF. Social conditions and self-management are more powerful determinants of health than access to care. Ann Intern Med. 1998;129(5):406–411. - PubMed
-
- Marmot MG. Understanding social inequalities in health. Perspect Biol Med. 2003;46(3 Suppl):S9–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
