

Hepatic profile analyses of tipranavir in Phase II and III clinical trials
- PMID: 20003457
- PMCID: PMC2803791
- DOI: 10.1186/1471-2334-9-203
Hepatic profile analyses of tipranavir in Phase II and III clinical trials
Abstract
Background: The risk and course of serum transaminase elevations (TEs) and clinical hepatic serious adverse event (SAE) development in ritonavir-boosted tipranavir (TPV/r) 500/200 mg BID recipients, who also received additional combination antiretroviral treatment agents in clinical trials (TPV/r-based cART), was determined.
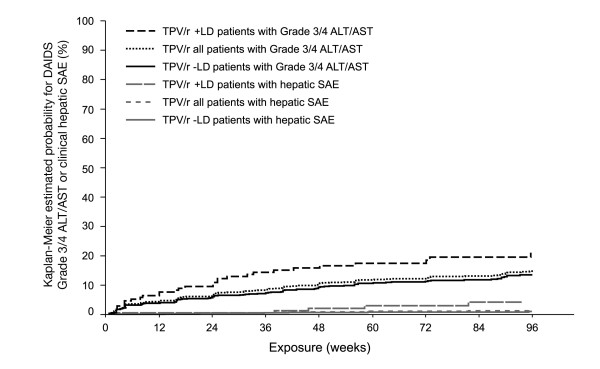
Methods: Aggregated transaminase and hepatic SAE data through 96 weeks of TPV/r-based cART from five Phase IIb/III trials were analyzed. Patients were categorized by the presence or absence of underlying liver disease (+LD or -LD). Kaplan-Meier (K-M) probability estimates for time-to-first US National Institutes of Health, Division of AIDS (DAIDS) Grade 3/4 TE and clinical hepatic SAE were determined and clinical actions/outcomes evaluated. Risk factors for DAIDS Grade 3/4 TE were identified through multivariate Cox regression statistical modeling.
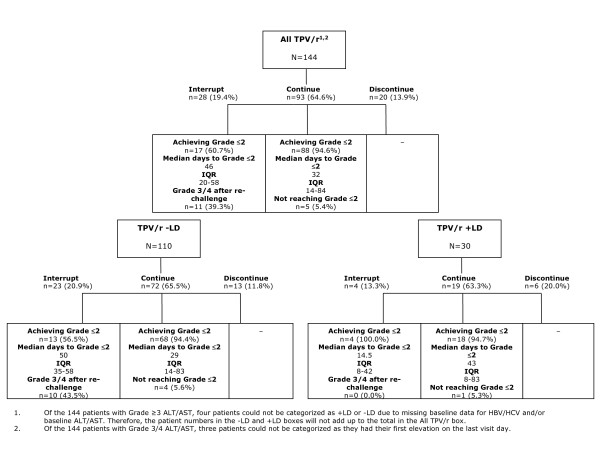
Results: Grade 3/4 TEs occurred in 144/1299 (11.1%) patients; 123/144 (85%) of these were asymptomatic; 84% of these patients only temporarily interrupted treatment or continued, with transaminase levels returning to Grade < or = 2. At 96 weeks of study treatment, the incidence of Grade 3/4 TEs was higher among the +LD (16.8%) than among the -LD (10.1%) patients. K-M analysis revealed an incremental risk for developing DAIDS Grade 3/4 TEs; risk was greatest through 24 weeks (6.1%), and decreasing thereafter (>24-48 weeks: 3.4%, >48 weeks-72 weeks: 2.0%, >72-96 weeks: 2.2%), and higher in +LD than -LD patients at each 24-week interval. Treatment with TPV/r, co-infection with hepatitis B and/or C, DAIDS grade >1 TE and CD4+ > 200 cells/mm3 at baseline were found to be independent risk factors for development of DAIDS Grade 3/4 TE; the hazard ratios (HR) were 2.8, 2.0, 2.1 and 1.5, respectively. Four of the 144 (2.7%) patients with Grade 3/4 TEs developed hepatic SAEs; overall, 14/1299 (1.1%) patients had hepatic SAEs including six with hepatic failure (0.5%). The K-M risk of developing hepatic SAEs through 96 weeks was 1.4%; highest risk was observed during the first 24 weeks and decreased thereafter; the risk was similar between +LD and -LD patients for the first 24 weeks (0.6% and 0.5%, respectively) and was higher for +LD patients, thereafter.
Conclusion: Through 96 weeks of TPV/r-based cART, DAIDS Grade 3/4 TEs and hepatic SAEs occurred in approximately 11% and 1% of TPV/r patients, respectively; most (84%) had no significant clinical implications and were managed without permanent treatment discontinuation. Among the 14 patients with hepatic SAE, 6 experienced hepatic failure (0.5%); these patients had profound immunosuppression and the rate appears higher among hepatitis co-infected patients. The overall probability of experiencing a hepatic SAE in this patient cohort was 1.4% through 96 weeks of treatment. Independent risk factors for DAIDS Grade 3/4 TEs include TPV/r treatment, co-infection with hepatitis B and/or C, DAIDS grade >1 TE and CD4+ > 200 cells/mm3 at baseline.
Trial registration: US-NIH Trial registration number: NCT00144170.
Figures
Similar articles
-
Tipranavir/Ritonavir (500/200 mg and 500/100 mg) Was Virologically Non-Inferior to Lopinavir/Ritonavir (400/100 mg) at Week 48 in Treatment-Naïve HIV-1-Infected Patients: A Randomized, Multinational, Multicenter Trial.PLoS One. 2016 Jan 5;11(1):e0144917. doi: 10.1371/journal.pone.0144917. eCollection 2016. PLoS One. 2016. PMID: 26730818 Free PMC article. Clinical Trial.
-
Hepatic safety of tipranavir plus ritonavir (TPV/r)-based antiretroviral combinations: effect of hepatitis virus co-infection and pre-existing fibrosis.J Antimicrob Chemother. 2009 Jan;63(1):178-83. doi: 10.1093/jac/dkn429. Epub 2008 Oct 24. J Antimicrob Chemother. 2009. PMID: 18952618
-
Efficacy, safety and tolerability of tipranavir coadministered with ritonavir in HIV-1-infected children and adolescents.AIDS. 2008 Sep 12;22(14):1789-98. doi: 10.1097/QAD.0b013e32830c481b. AIDS. 2008. PMID: 18753862 Free PMC article. Clinical Trial.
-
Intracranial hemorrhage and liver-associated deaths associated with tipranavir/ritonavir: review of cases from the FDA's Adverse Event Reporting System.AIDS Patient Care STDS. 2008 Nov;22(11):843-50. doi: 10.1089/apc.2008.0043. AIDS Patient Care STDS. 2008. PMID: 19025478 Review.
-
Tipranavir: the first nonpeptidic protease inhibitor for the treatment of protease resistance.Clin Ther. 2007 Nov;29(11):2309-18. doi: 10.1016/j.clinthera.2007.11.007. Clin Ther. 2007. PMID: 18158073 Review.
Cited by
-
Incidence and risk factors for liver enzymes elevations in highly treatment-experienced patients switching from enfuvirtide to raltegravir: a sub-study of the ANRS-138 EASIER trial.AIDS Res Ther. 2016 Apr 2;13:17. doi: 10.1186/s12981-016-0101-3. eCollection 2016. AIDS Res Ther. 2016. PMID: 27042193 Free PMC article. Clinical Trial.
-
Liver injury correlates with biomarkers of autoimmunity and disease activity and represents an organ system involvement in patients with systemic lupus erythematosus.Clin Immunol. 2015 Oct;160(2):319-27. doi: 10.1016/j.clim.2015.07.001. Epub 2015 Jul 6. Clin Immunol. 2015. PMID: 26160213 Free PMC article.
-
Human immunodeficiency virus and liver disease forum 2012.Hepatology. 2014 Jan;59(1):307-17. doi: 10.1002/hep.26638. Epub 2013 Nov 22. Hepatology. 2014. PMID: 23904401 Free PMC article.
-
Liver safety assessment in special populations (hepatitis B, C, and oncology trials).Drug Saf. 2014 Nov;37 Suppl 1(Suppl 1):S57-62. doi: 10.1007/s40264-014-0186-3. Drug Saf. 2014. PMID: 25352328 Free PMC article. Review.
References
-
- Cooper D, Hall D, Jayaweera D. Baseline phenotypic susceptibility to tipranavir/ritonavir is retained in isolates from patients with multiple protease inhibitor experience (BI 1182.52). [abstract 596] Presented at: 10th Conference on Retroviruses and Opportunistic Infections; Boston. 2003.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
