

Oral contraceptive use and bone density in adolescent and young adult women
- PMID: 20004271
- PMCID: PMC2822656
- DOI: 10.1016/j.contraception.2009.07.001
Oral contraceptive use and bone density in adolescent and young adult women
Abstract
Background: Most of the millions of oral contraceptive (OC) users are under 30 years of age and in the critical period for bone mass accrual.
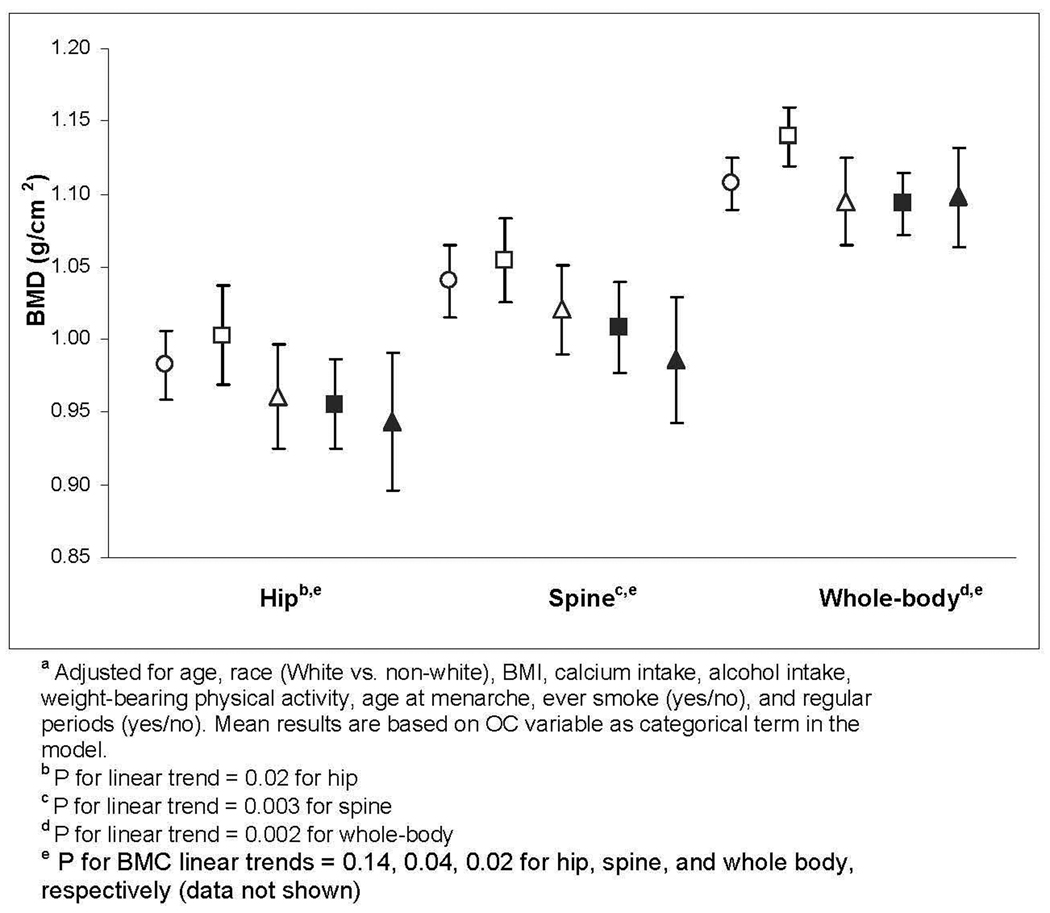
Study design: This cross-sectional study of 606 women aged 14-30 years examined both OC duration and estrogen dose and their association with bone mineral density (BMD) at the hip, spine, and whole body (dual-energy X-ray absorptiometry).
Results: Of 389 OC users and 217 nonusers enrolled, 50% were adolescents (14-18 years). Of OC users, 38% used "low-dose" OCs [<30 mcg ethinyl estradiol (EE)]. In adolescents, mean BMD differed by neither OC duration nor EE dose. However, 19- to 30-year-old women's mean BMD was lower with longer OC use for spine and whole body (p=.004 and p=.02, respectively) and lowest for >12 months of low-dose OCs for the hip, spine and whole body (p=.02, .003 and .002, respectively).
Conclusions: Prolonged use of today's OCs, particularly <30 mcg EE, may adversely impact young adult women's bone density while using these agents.
Figures
Similar articles
-
Oral contraceptive use and bone density change in adolescent and young adult women: a prospective study of age, hormone dose, and discontinuation.J Clin Endocrinol Metab. 2011 Sep;96(9):E1380-7. doi: 10.1210/jc.2010-3027. Epub 2011 Jul 13. J Clin Endocrinol Metab. 2011. PMID: 21752879 Free PMC article.
-
Lack of relationship between hip and spine bone mineral density and oral contraceptive use.Eur J Clin Invest. 1993 Feb;23(2):108-11. doi: 10.1111/j.1365-2362.1993.tb00749.x. Eur J Clin Invest. 1993. PMID: 8462619
-
Age at first oral contraceptive use as a major determinant of vertebral bone mass in female endurance athletes.Bone. 2004 Oct;35(4):836-41. doi: 10.1016/j.bone.2004.05.017. Bone. 2004. PMID: 15454090
-
Oral contraceptives for the prevention of osteoporosis.J Reprod Med. 1993 Dec;38(12 Suppl):1015-20. J Reprod Med. 1993. PMID: 8120858 Review.
-
Bone-sparing properties of oral contraceptives.Am J Obstet Gynecol. 1996 Jan;174(1 Pt 1):15-20. doi: 10.1016/s0002-9378(96)70366-6. Am J Obstet Gynecol. 1996. PMID: 8571999 Review.
Cited by
-
Oral contraceptive use and bone density change in adolescent and young adult women: a prospective study of age, hormone dose, and discontinuation.J Clin Endocrinol Metab. 2011 Sep;96(9):E1380-7. doi: 10.1210/jc.2010-3027. Epub 2011 Jul 13. J Clin Endocrinol Metab. 2011. PMID: 21752879 Free PMC article.
-
Hormonal Contraception and Bone Metabolism: Emerging Evidence from a Systematic Review and Meta-Analysis of Studies on Post-Pubertal and Reproductive-Age Women.Pharmaceuticals (Basel). 2025 Jan 8;18(1):61. doi: 10.3390/ph18010061. Pharmaceuticals (Basel). 2025. PMID: 39861124 Free PMC article. Review.
-
Infant milk feeding influences adult bone health: a prospective study from birth to 32 years.PLoS One. 2011 Apr 27;6(4):e19068. doi: 10.1371/journal.pone.0019068. PLoS One. 2011. PMID: 21556368 Free PMC article.
-
Oral contraceptive use and bone.Curr Osteoporos Rep. 2011 Mar;9(1):6-11. doi: 10.1007/s11914-010-0037-9. Curr Osteoporos Rep. 2011. PMID: 21104044 Review.
-
Oral contraceptive use, bone mineral density, and bone turnover markers over 12 months in college-aged females.J Bone Miner Metab. 2020 Jul;38(4):544-554. doi: 10.1007/s00774-019-01081-1. Epub 2020 Jan 25. J Bone Miner Metab. 2020. PMID: 31983034 Free PMC article.
References
-
- Chandra A, Martinez GM, Mosher WD, Abma JC, Jones J. Fertility, family planning, and reproductive health of U.S. women: data from the 2002 National Survey of Family Growth. Vital Health Stat. 2005;23:1–160. - PubMed
-
- Martins SL, Curtis KM, Glasier AF. Combined hormonal contraception and bone health: a systematic review. Contraception. 2006;73:445–469. - PubMed
-
- Hartard M, Kleinmond C, Wiseman M, Weissenbacher ER, Felsenberg D, Erben RG. Detrimental effect of oral contraceptives on parameters of bone mass and geometry in a cohort of 248 young women. Bone. 2007;40:444–450. - PubMed
-
- Polatti F, Perotti F, Filippa N, Gallina D, Nappi RE. Bone mass and long-term monophasic oral contraceptive treatment in young women. Contraception. 1995;51:221–224. - PubMed
-
- Register TC, Jayo MJ, Jerome CP. Oral contraceptive treatment inhibits the normal acquisition of bone mineral in skeletally immature young adult female monkeys. Osteoporos Int. 1997;7:348–353. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
