

ORAI1 deficiency and lack of store-operated Ca2+ entry cause immunodeficiency, myopathy, and ectodermal dysplasia
- PMID: 20004786
- PMCID: PMC2829767
- DOI: 10.1016/j.jaci.2009.10.007
ORAI1 deficiency and lack of store-operated Ca2+ entry cause immunodeficiency, myopathy, and ectodermal dysplasia
Abstract
Background: Defects in the development or activation of T cells result in immunodeficiency associated with severe infections early in life. T-cell activation requires Ca2+ influx through Ca2+-release activated Ca2+ (CRAC) channels encoded by the gene ORAI1.
Objective: Investigation of the genetic causes and the clinical phenotype of immunodeficiency in patients with impaired Ca2+ influx and CRAC channel function.
Methods: DNA sequence analysis for mutations in the genes ORAI1, ORAI2, ORAI3, and stromal interaction molecule (STIM) 1 and 2, as well as mRNA and protein expression analysis of ORAI1 in immunodeficient patients. Immunohistochemical analysis of ORAI1 tissue distribution in healthy human donors.
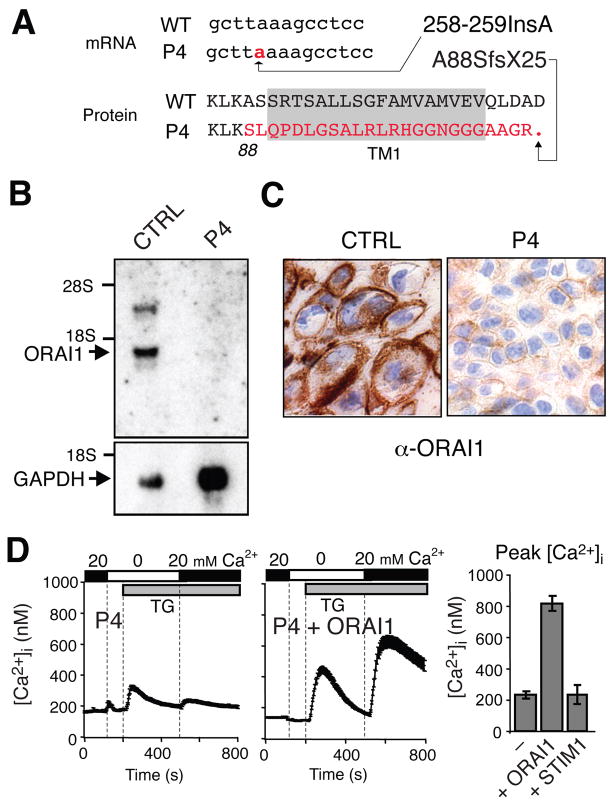
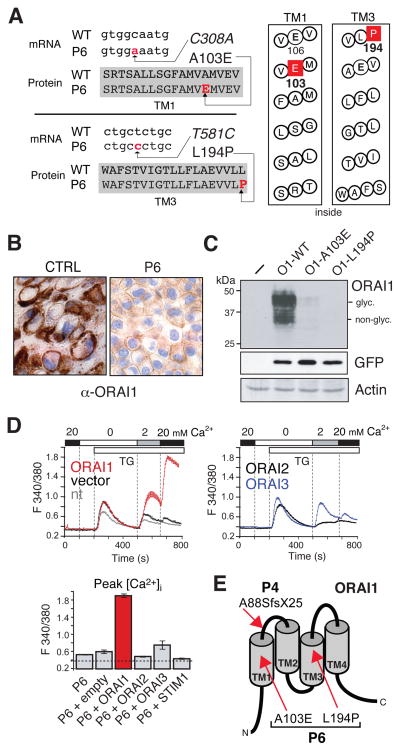
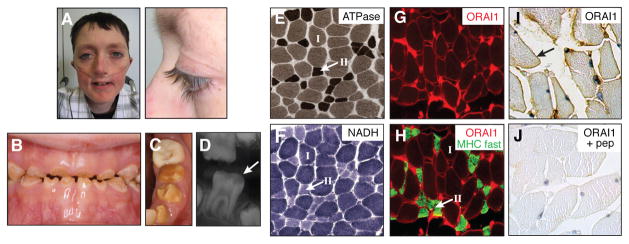
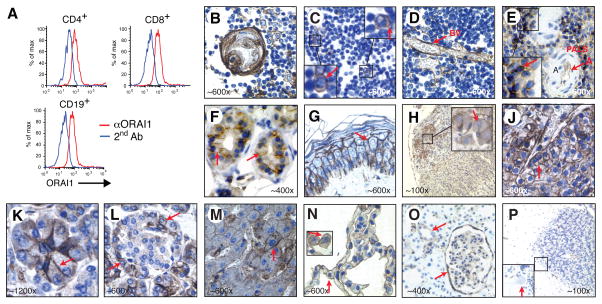
Results: We identified mutations in ORAI1 in patients from 2 unrelated families. One patient is homozygous for a frameshift nonsense mutation in ORAI1 (ORAI1-A88SfsX25), and a second patient is compound heterozygous for 2 missense mutations in ORAI1 (ORAI1-A103E/L194P). All 3 mutations abolish ORAI1 expression and impair Ca2+ influx and CRAC channel function. The clinical syndrome associated with ORAI1 deficiency is characterized by immunodeficiency with a defect in the function but not in the development of lymphocytes, congenital myopathy, and anhydrotic ectodermal dysplasia with a defect in dental enamel calcification. In contrast with the limited clinical phenotype, we found ORAI1 protein expression in a wide variety of cell types and organs.
Conclusion: Ca2+ influx through ORAI1 is crucial for lymphocyte function in vivo. Despite almost ubiquitous ORAI1 expression, the channel has a nonredundant role in only a few cell types judging from the limited clinical phenotype in ORAI1-deficient patients.
Conflict of interest statement
Disclosure of potential conflict of interest: A. Rao and S. Feske are scientific co-founders and members of the scientific advisory board of CalciMedica. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Fischer A. Human primary immunodeficiency diseases. Immunity. 2007;27:835–45. - PubMed
-
- Feske S. Calcium signalling in lymphocyte activation and disease. Nat Rev Immunol. 2007;7:690–702. - PubMed
-
- Lewis RS. The molecular choreography of a store-operated calcium channel. Nature. 2007;446:284–7. - PubMed
-
- Prakriya M, Feske S, Gwack Y, Srikanth S, Rao A, Hogan PG. Orai1 is an essential pore subunit of the CRAC channel. Nature. 2006;443:230–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
