

Has the frequency of bleeding changed over time for patients presenting with an acute coronary syndrome? The global registry of acute coronary events
- PMID: 20007159
- PMCID: PMC2838680
- DOI: 10.1093/eurheartj/ehp499
Has the frequency of bleeding changed over time for patients presenting with an acute coronary syndrome? The global registry of acute coronary events
Abstract
Aims: To determine whether changes in practice, over time, are associated with altered rates of major bleeding in acute coronary syndromes (ACS).
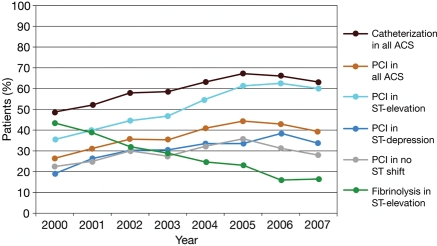
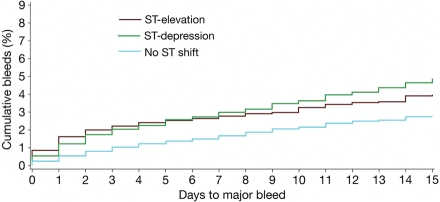
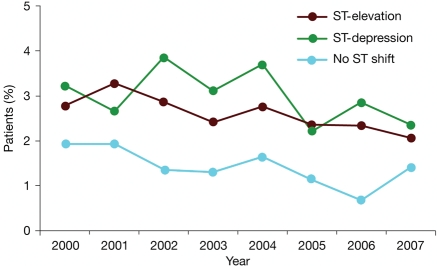
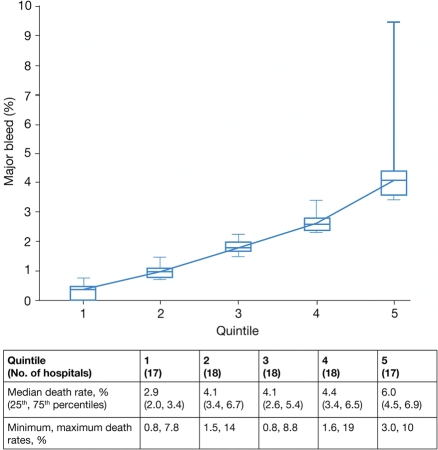
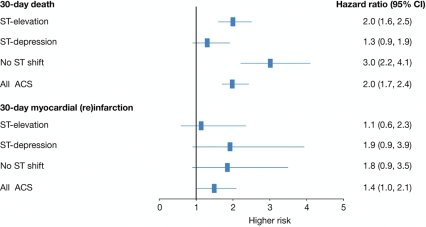
Methods and results: Patients from the Global Registry of Acute Coronary Events were enrolled between 2000 and 2007. The main outcome measures were frequency of major bleeding, including haemorrhagic stroke, over time, after adjustment for patient characteristics, and impact of major bleeding on death and myocardial infarction. Of the 50 947 patients, 2.3% sustained a major bleed; almost half of these presented with ST-elevation ACS (44%, 513). Despite changes in antithrombotic therapy (increasing use of low molecular weight heparin, P < 0.0001), thienopyridines (P < 0.0001), and percutaneous coronary interventions (P < 0.0001), frequency of major bleeding for all ACS patients decreased (2.6 to 1.8%; P < 0.0001). Most decline was seen in ST-elevation ACS (2.9 to 2.1%, P = 0.02). The overall decline remained after adjustment for patient characteristics and treatments (P = 0.002, hazard ratio 0.94 per year, 95% confidence interval 0.91-0.98). Hospital characteristics were an independent predictor of bleeding (P < 0.0001). Patients who experienced major bleeding were at increased risk of death within 30 days from admission, even after adjustment for baseline variables.
Conclusion: Despite increasing use of more intensive therapies, there was a decline in the rate of major bleeding associated with changes in clinical practice. However, individual hospital characteristics remain an important determinant of the frequency of major bleeding.
Figures
Comment in
-
A reduction in bleeding in acute coronary syndromes? Let's not rain on the parade!Eur Heart J. 2010 Mar;31(6):640-1. doi: 10.1093/eurheartj/ehp577. Epub 2009 Dec 27. Eur Heart J. 2010. PMID: 20038514 No abstract available.
References
-
- Eikelboom JW, Mehta SR, Anand SS, Xie C, Fox KA, Yusuf S. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation. 2006;114:774–782. - PubMed
-
- Rao SV, O'Grady K, Pieper KS, Granger CB, Newby LK, Van de Werf F, Mahaffey KW, Califf RM, Harrington RA. Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes. Am J Cardiol. 2005;96:1200–1206. - PubMed
-
- Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A, Fernandez-Aviles F, Fox KA, Hasdai D, Ohman EM, Wallentin L, Wijns W, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Kristensen SD, Widimsky P, McGregor K, Sechtem U, Tendera M, Hellemans I, Gomez JL, Silber S, Funck-Brentano C, Andreotti F, Benzer W, Bertrand M, Betriu A, Desutter J, Falk V, Ortiz AF, Gitt A, Hasin Y, Huber K, Kornowski R, Lopez-Sendon J, Morais J, Nordrehaug JE, Steg PG, Thygesen K, Tubaro M, Turpie AG, Verheugt F, Windecker S. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology. Eur Heart J. 2007;28:1598–1660. - PubMed
-
- Fox KA, Steg PG, Eagle KA, Goodman SG, Anderson FA, Jr, Granger CB, Flather MD, Budaj A, Quill A, Gore JM. Decline in rates of death and heart failure in acute coronary syndromes, 1999–2006. J Am Med Assoc. 2007;297:1892–1900. - PubMed
-
- Yusuf S, Mehta SR, Chrolavicius S, Afzal R, Pogue J, Granger CB, Budaj A, Peters RJ, Bassand JP, Wallentin L, Joyner C, Fox KA. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med. 2006;354:1464–1476. - PubMed
