

Real-time continuous glucose monitoring in critically ill patients: a prospective randomized trial
- PMID: 20007948
- PMCID: PMC2827490
- DOI: 10.2337/dc09-1352
Real-time continuous glucose monitoring in critically ill patients: a prospective randomized trial
Abstract
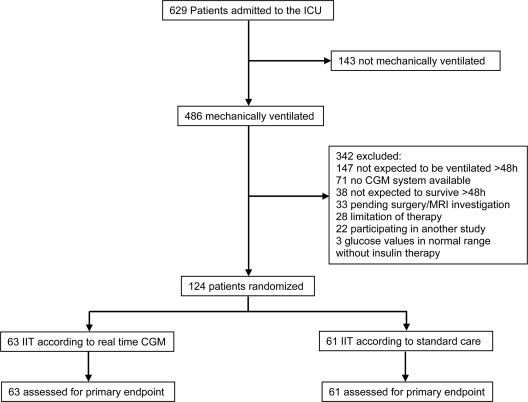
OBJECTIVE To evaluate the impact of real-time continuous glucose monitoring (CGM) on glycemic control and risk of hypoglycemia in critically ill patients. RESEARCH DESIGN AND METHODS A total 124 patients receiving mechanical ventilation were randomly assigned to the real-time CGM group (n = 63; glucose values given every 5 min) or to the control group (n = 61; selective arterial glucose measurements according to an algorithm; simultaneously blinded CGM) for 72 h. Insulin infusion rates were guided according to the same algorithm in both groups. The primary end point was percentage of time at a glucose level <110 mg/dl. Secondary end points were mean glucose levels and rate of severe hypoglycemia (<40 mg/dl). RESULTS Percentage of time at a glucose level <110 mg/dl (59.0 +/- 20 vs. 55.0 +/- 18% in the control group, P = 0.245) and the mean glucose level (106 +/- 18 vs. 111 +/- 10 mg/dl in the control group, P = 0.076) could not be improved using real-time CGM. The rate of severe hypoglycemia was lower in the real-time CGM group (1.6 vs. 11.5% in the control group, P = 0.031). CGM reduced the absolute risk of severe hypoglycemia by 9.9% (95% CI 1.2-18.6) with a number needed to treat of 10.1 (95% CI 5.4-83.3). CONCLUSIONS In critically ill patients, real-time CGM reduces hypoglycemic events but does not improve glycemic control compared with intensive insulin therapy guided by an algorithm.
Figures
References
-
- Finney SJ, Zekveld C, Elia A, Evans TW: Glucose control and mortality in critically ill patients. JAMA 2003;290:2041–2047 - PubMed
-
- Krinsley JS: Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc 2003;78:1471–1478 - PubMed
-
- van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R: Intensive insulin therapy in the critically ill patients. N Engl J Med 2001;345:1359–1367 - PubMed
-
- Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, Van Wijngaerden E, Bobbaers H, Bouillon R: Intensive insulin therapy in the medical ICU. N Engl J Med 2006;354:449–461 - PubMed
-
- Vlasselaers D, Milants I, Desmet L, Wouters PJ, Vanhorebeek I, van den Heuvel I, Mesotten D, Casaer MP, Meyfroidt G, Ingels C, Muller J, Van Cromphaut S, Schetz M, Van den Berghe G: Intensive insulin therapy for patients in paediatric intensive care: a prospective, randomised controlled study. Lancet 2009;373:547–556 - PubMed
