

Baroreflex control of muscle sympathetic nerve activity: a nonpharmacological measure of baroreflex sensitivity
- PMID: 20008270
- PMCID: PMC2838548
- DOI: 10.1152/ajpheart.00924.2009
Baroreflex control of muscle sympathetic nerve activity: a nonpharmacological measure of baroreflex sensitivity
Abstract
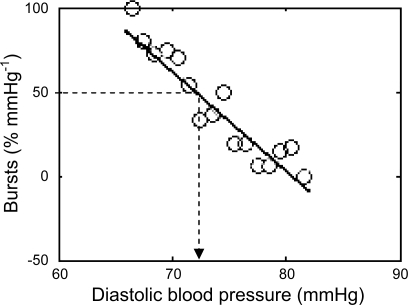
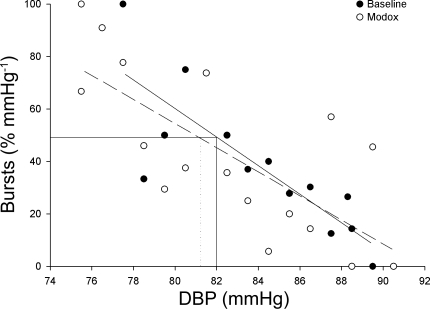
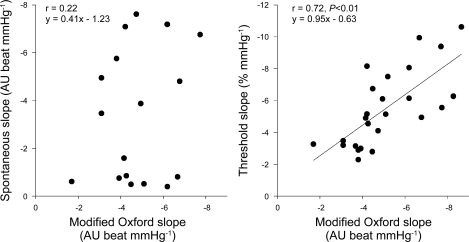
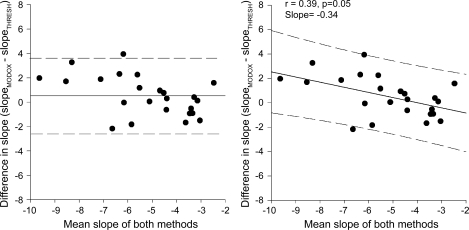
The sensitivity of baroreflex control of sympathetic nerve activity (SNA) represents the responsiveness of SNA to changes in blood pressure. In a slightly different analysis, the baroreflex threshold measures the probability of whether a sympathetic burst will occur at a given diastolic blood pressure. We hypothesized that baroreflex threshold analysis could be used to estimate the sensitivity of the sympathetic baroreflex measured by the pharmacological modified Oxford test. We compared four measures of sympathetic baroreflex sensitivity in 25 young healthy participants: the "gold standard" modified Oxford analysis (nitroprusside and phenylephrine), nonbinned spontaneous baroreflex analysis, binned spontaneous baroreflex analysis, and threshold analysis. The latter three were performed during a quiet baseline period before pharmacological intervention. The modified Oxford baroreflex sensitivity was significantly related to the threshold slope (r = 0.71, P < 0.05) but not to the binned (1 mmHg bins) and the nonbinned spontaneous baroreflex sensitivity (r = 0.22 and 0.36, respectively, P > 0.05), which included burst area. The threshold analysis was also performed during the modified Oxford manipulation. Interestingly, we found that the threshold analysis results were not altered by the vasoactive drugs infused for the modified Oxford. We conclude that the noninvasive threshold analysis technique can be used as an indicator of muscle SNA baroreflex sensitivity as assessed by the modified Oxford technique. Furthermore, the modified Oxford method does not appear to alter the properties of the baroreflex.
Figures
References
-
- Bertinieri G, Di Rienzo M, Cavallazzi A, Ferrari AU, Pedotti A, Mancia G. Evaluation of baroreceptor reflex by blood pressure monitoring in unanesthetized cats. Am J Physiol Heart Circ Physiol 254: H377–H383, 1988 - PubMed
-
- Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1: 307–310, 1986 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials