

The arterial reservoir pressure increases with aging and is the major determinant of the aortic augmentation index
- PMID: 20008272
- PMCID: PMC2822572
- DOI: 10.1152/ajpheart.00875.2009
The arterial reservoir pressure increases with aging and is the major determinant of the aortic augmentation index
Abstract
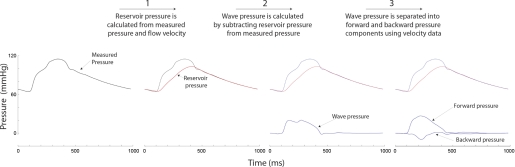
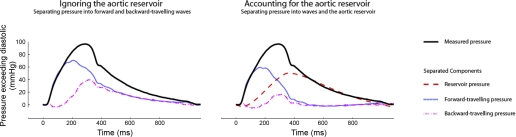
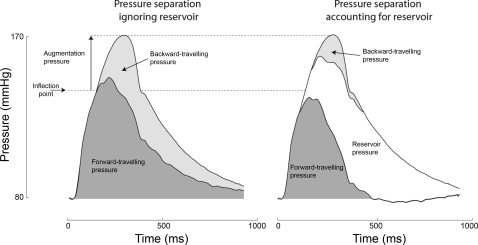
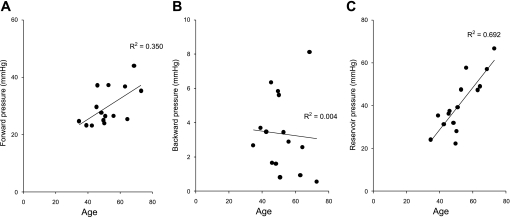
The augmentation index predicts cardiovascular mortality and is usually explained as a distally reflected wave adding to the forward wave generated by systole. We propose that the capacitative properties of the aorta (the arterial reservoir) also contribute significantly to the augmentation index and have calculated the contribution of the arterial reservoir, independently of wave reflection, and assessed how these contributions change with aging. In 15 subjects (aged 53 +/- 10 yr), we measured pressure and Doppler velocity simultaneously in the proximal aorta using intra-arterial wires. We calculated the components of augmentation pressure in two ways: 1) into forward and backward (reflected) components by established separation methods, and 2) using an approach that accounts for an additional reservoir component. When the reservoir was ignored, augmentation pressure (22.7 +/- 13.9 mmHg) comprised a small forward wave (peak pressure = 6.5 +/- 9.4 mmHg) and a larger backward wave (peak pressure = 16.2 +/- 7.6 mmHg). After we took account of the reservoir, the contribution to augmentation pressure of the backward wave was reduced by 64% to 5.8 +/- 4.4 mmHg (P < 0.001), forward pressure was negligible, and reservoir pressure was the largest component (peak pressure = 19.8 +/- 9.3 mmHg). With age, reservoir pressure increased progressively (9.9 mmHg/decade, r = 0.69, P < 0.001). In conclusion, the augmentation index is principally determined by aortic reservoir function and other elastic arteries and only to a minor extent by reflected waves. Reservoir function rather than wave reflection changes markedly with aging, which accounts for the age-related changes in the aortic pressure waveform.
Figures
References
-
- Baksi AJ, Treibel TA, Davies JE, Hadjiloizou NF, Parker KH, Francis DP, Mayet J, Hughes AD. A meta-analysis of mechanism of blood pressure change with aging. J Am Coll Cardiol 54: 2087–2092, 2009 - PubMed
-
- Broemser PR. Ueber die Messung des Schlagvolumens des Herzens auf unblutigem Weg. Z Biol 90: 467–507, 1930
-
- Cameron JD, McGrath BP, Dart AM. Use of radial artery applanation tonometry and a generalized transfer function to determine aortic pressure augmentation in subjects with treated hypertension. J Am Coll Cardiol 32: 1214–1220, 1998 - PubMed
-
- Chen CH, Nevo E, Fetics B, Pak PH, Yin FC, Maughan WL, Kass DA. Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure. Validation of generalized transfer function. Circulation 95: 1827–1836, 1997 - PubMed
-
- Chen CH, Ting CT, Nussbacher A, Nevo E, Kass DA, Pak P, Wang SP, Chang MS, Yin FC. Validation of carotid artery tonometry as a means of estimating augmentation index of ascending aortic pressure. Hypertension 27: 168–175, 1996 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical