

Reversible or irreversible remodeling in pulmonary arterial hypertension
- PMID: 20008280
- PMCID: PMC2993084
- DOI: 10.1165/rcmb.2009-0389TR
Reversible or irreversible remodeling in pulmonary arterial hypertension
Abstract
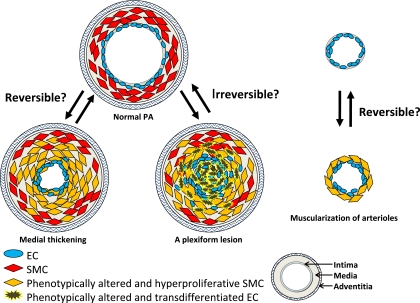
Vascular remodeling is an important pathological feature of pulmonary arterial hypertension (PAH), which leads to increased pulmonary vascular resistance, with marked proliferation of pulmonary artery smooth muscle cells (SMC) and/or endothelial cells (EC). Successful treatment of experimental PAH with a platelet-derived growth factor (PDGF) receptor tyrosine kinase inhibitor offers the perspective of "reverse remodeling" (i.e., the regression of established pulmonary vascular lesions). Here we ask the question: which forms of pulmonary vascular remodeling are reversible and can such remodeling caused by angiogenic proliferation of EC be reversed? It is important to emphasize that the report showing reduction of vascular remodeling by PDGF receptor tyrosine kinase inhibitor showed only a reduction of the pulmonary artery muscularization in chronic hypoxia and monocrotaline models, which lack the feature of clustered proliferated EC in the lumen of pulmonary arteries. The regression of vascular muscularization is an important manifestation, whereby proliferative adult SMC convert back to a nonproliferative state. In contrast, in vitro experiments assessing the contribution of EC to the development of PAH demonstrated that phenotypically altered EC generated as a consequence of a vascular endothelial growth factor receptor blockade did not reverse to normal EC. Whereas it is suggested that the proliferative state of SMC may be reversible, it remains unknown whether phenotypically altered EC can switch back to a normal monolayer-forming EC. This article reviews the pathogenetic concepts of severe PAH and explains the many forms in PAH with reversible or irreversible remodeling.
Figures
References
-
- Humbert M, Morrell NW, Archer SL, Stenmark KR, MacLean MR, Lang IM, Christman BW, Weir EK, Eickelberg O, Voelkel NF, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:13S–24S. - PubMed
-
- Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med 2004;351:1425–1436. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
