

Pediatric specialists' beliefs about gastroesophageal reflux disease in premature infants
- PMID: 20008431
- PMCID: PMC2805060
- DOI: 10.1542/peds.2008-3841
Pediatric specialists' beliefs about gastroesophageal reflux disease in premature infants
Abstract
Background: Wide variation exists in the treatment of suspected gastroesophageal reflux disease (GERD) in premature infants; it is unknown to what degree diagnosis and treatment are affected by the treating physician's medical specialty or interpretation of the medical literature.
Methods: This study involved an online survey of board-certified neonatologists, pediatric pulmonologists, and pediatric gastroenterologists about their beliefs regarding the symptoms, diagnosis, and treatment of GERD in premature infants in the NICU on the basis of both clinical impression and interpretation of the literature.
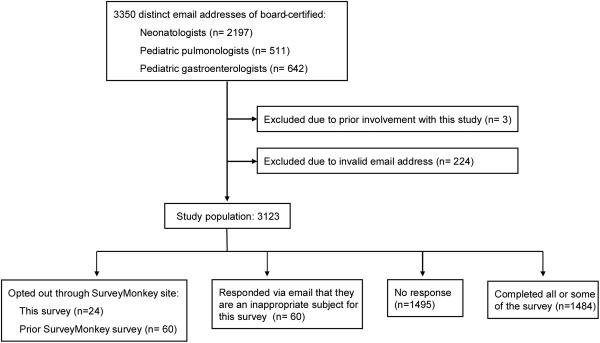
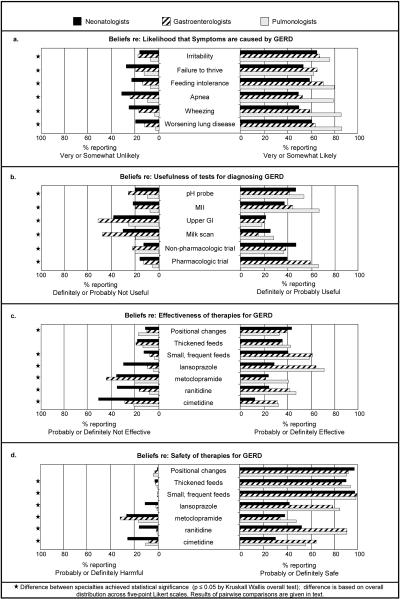
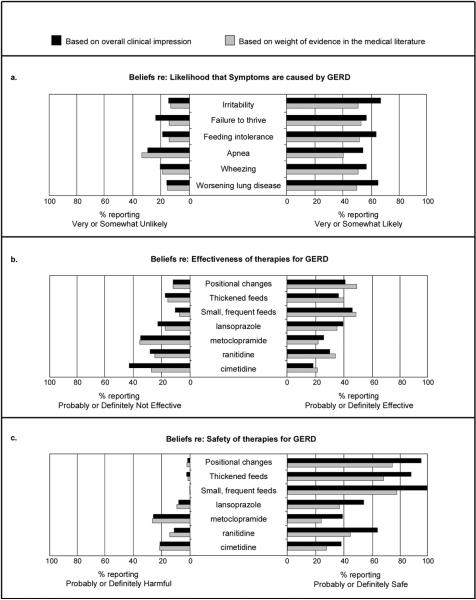
Results: A total of 1021 neonatologists, 232 pediatric pulmonologists, and 222 pediatric gastroenterologists participated in the study (47.5% response rate). There was disagreement among specialists in nearly all aspects of the survey. Pulmonologists were most likely to report that respiratory symptoms are caused by GERD (P < .001). Neonatologists were least likely to report that a therapeutic trial of pharmacologic agents would be useful for diagnosing GERD (P < .001) or that lansoprazole, ranitidine, or cimetidine are safe or effective (P < .001). No pharmacologic therapy had >50% of respondents supporting its effectiveness. There was moderate correlation between physician belief based on the medical literature and belief based on clinical impression (Spearman rank correlation: 0.47-0.75). For therapies supported by multiple meta-analyses in infants versus therapies with few infant trials, physicians rated the evidence for effectiveness similarly.
Conclusions: There is wide variation among pediatric specialists regarding beliefs about GERD in premature infants, as well as about the weight of evidence in the medical literature for this patient population. Physician beliefs do not seem to be driven by the degree of evidence in the neonatal literature. With no agreed-on standard of care in the setting of widespread use of antireflux medications, greater understanding is needed about the ways physicians form clinical impressions, access and process medical evidence, and apply it to patient care.
Figures
Similar articles
-
Chronic laryngitis associated with gastroesophageal reflux: prospective assessment of differences in practice patterns between gastroenterologists and ENT physicians.Am J Gastroenterol. 2006 Mar;101(3):470-8. doi: 10.1111/j.1572-0241.2006.00502.x. Am J Gastroenterol. 2006. PMID: 16542282
-
Discerning differences: gastroesophageal reflux and gastroesophageal reflux disease in infants.Adv Neonatal Care. 2004 Aug;4(4):235-47. doi: 10.1016/j.adnc.2004.05.006. Adv Neonatal Care. 2004. PMID: 15368216 Review.
-
Development of a Core Outcome Set for Infant Gastroesophageal Reflux Disease.J Pediatr Gastroenterol Nutr. 2019 May;68(5):655-661. doi: 10.1097/MPG.0000000000002245. J Pediatr Gastroenterol Nutr. 2019. PMID: 31022093
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
[Gastroesophageal reflux in premature: a case report].Pan Afr Med J. 2016 Dec 20;25:243. doi: 10.11604/pamj.2016.25.243.10497. eCollection 2016. Pan Afr Med J. 2016. PMID: 28293359 Free PMC article. Review. French.
Cited by
-
Neonatal Histamine-2 Receptor Antagonist and Proton Pump Inhibitor Treatment at United States Children's Hospitals.J Pediatr. 2016 Jul;174:63-70.e3. doi: 10.1016/j.jpeds.2016.03.059. Epub 2016 Apr 27. J Pediatr. 2016. PMID: 27131401 Free PMC article.
-
Gastroesophageal Reflux Disease in the Neonatal Intensive Care Unit Infant: Who Needs to Be Treated and What Approach Is Beneficial?Pediatr Clin North Am. 2019 Apr;66(2):461-473. doi: 10.1016/j.pcl.2018.12.012. Epub 2019 Feb 1. Pediatr Clin North Am. 2019. PMID: 30819348 Free PMC article. Review.
-
Use of Gastroesophageal Reflux Medications in Premature Infants After NICU Discharge.Pediatrics. 2016 Dec;138(6):e20161977. doi: 10.1542/peds.2016-1977. Pediatrics. 2016. PMID: 27940703 Free PMC article.
-
Gastroesophageal reflux disease in children: What's new right now?World J Gastrointest Endosc. 2023 Mar 16;15(3):84-102. doi: 10.4253/wjge.v15.i3.84. World J Gastrointest Endosc. 2023. PMID: 37034973 Free PMC article. Review.
-
Practice Variance, Prevalence, and Economic Burden of Premature Infants Diagnosed With GERD.Hosp Pediatr. 2013 Oct;3(4):335-41. doi: 10.1542/hpeds.2013-0036. Hosp Pediatr. 2013. PMID: 24435191 Free PMC article.
References
-
- Freed GL. Society for Pediatric Research--2007 presidential address: expanding the research continuum--from bench to implementation. Pediatr Res. 2007;62(3):370–3. - PubMed
-
- Marino AJ, et al. The incidence of gastroesophageal reflux in preterm infants. J Perinatol. 1995;15(5):369–71. - PubMed
-
- Di Fiore JM, et al. Apnea is not prolonged by acid gastroesophageal reflux in preterm infants. Pediatrics. 2005;116(5):1059–63. - PubMed
-
- Heine RG, et al. Clinical predictors of pathological gastro-oesophageal reflux in infants with persistent distress. J Paediatr Child Health. 2006;42(3):134–9. - PubMed
