

Provision of spiritual care to patients with advanced cancer: associations with medical care and quality of life near death
- PMID: 20008625
- PMCID: PMC2815706
- DOI: 10.1200/JCO.2009.24.8005
Provision of spiritual care to patients with advanced cancer: associations with medical care and quality of life near death
Abstract
Purpose: To determine whether spiritual care from the medical team impacts medical care received and quality of life (QoL) at the end of life (EoL) and to examine these relationships according to patient religious coping.
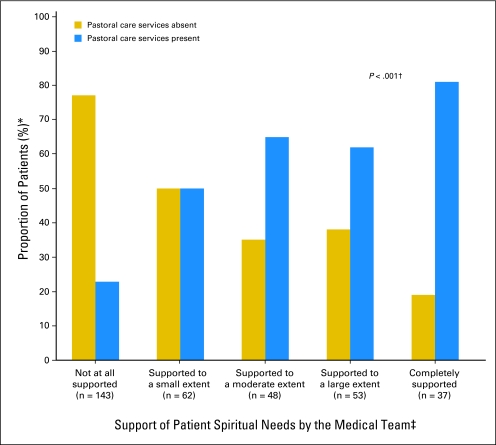
Patients and methods: Prospective, multisite study of patients with advanced cancer from September 2002 through August 2008. We interviewed 343 patients at baseline and observed them (median, 116 days) until death. Spiritual care was defined by patient-rated support of spiritual needs by the medical team and receipt of pastoral care services. The Brief Religious Coping Scale (RCOPE) assessed positive religious coping. EoL outcomes included patient QoL and receipt of hospice and any aggressive care (eg, resuscitation). Analyses were adjusted for potential confounders and repeated according to median-split religious coping.
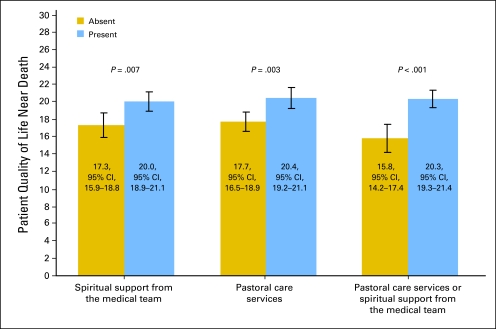
Results: Patients whose spiritual needs were largely or completely supported by the medical team received more hospice care in comparison with those not supported (adjusted odds ratio [AOR] = 3.53; 95% CI, 1.53 to 8.12, P = .003). High religious coping patients whose spiritual needs were largely or completely supported were more likely to receive hospice (AOR = 4.93; 95% CI, 1.64 to 14.80; P = .004) and less likely to receive aggressive care (AOR = 0.18; 95% CI, 0.04 to 0.79; P = .02) in comparison with those not supported. Spiritual support from the medical team and pastoral care visits were associated with higher QOL scores near death (20.0 [95% CI, 18.9 to 21.1] v 17.3 [95% CI, 15.9 to 18.8], P = .007; and 20.4 [95% CI, 19.2 to 21.1] v 17.7 [95% CI, 16.5 to 18.9], P = .003, respectively).
Conclusion: Support of terminally ill patients' spiritual needs by the medical team is associated with greater hospice utilization and, among high religious copers, less aggressive care at EoL. Spiritual care is associated with better patient QoL near death.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Spiritual care in patients with advanced cancer: what does it imply?J Clin Oncol. 2010 Jul 10;28(20):e332; author reply e333. doi: 10.1200/JCO.2010.28.4612. Epub 2010 May 10. J Clin Oncol. 2010. PMID: 20458027 No abstract available.
References
-
- Reynolds MA. Hope in adults, ages 20-59, with advanced stage cancer. Palliat Support Care. 2008;6:259–264. - PubMed
-
- Saleh US, Brockopp DY. Hope among patients with cancer hospitalized for bone marrow transplantation: A phenomenologic study. Cancer Nurs. 2001;24:308–314. - PubMed
-
- Fanos JH, Gelinas DF, Foster RS, et al. Hope in palliative care: From narcissism to self-transcendence in amyotrophic lateral sclerosis. J Palliat Med. 2008;11:470–475. - PubMed
-
- McClain CS, Rosenfeld B, Breitbart W. Effect of spiritual well-being on end-of-life despair in terminally-ill cancer patients. Lancet. 2003;361:1603–1607. - PubMed
-
- Gall TL, Cornblat MW. Breast cancer survivors give voice: A qualitative analysis of spiritual factors in long-term adjustment. Psychooncology. 2002;11:524–535. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
