

Quantitative template for subtyping primary progressive aphasia
- PMID: 20008661
- PMCID: PMC2796598
- DOI: 10.1001/archneurol.2009.288
Quantitative template for subtyping primary progressive aphasia
Abstract
Background: The syndrome of primary progressive aphasia (PPA) is diagnosed when a gradual failure of word usage or comprehension emerges as the principal feature of a neurodegenerative disease.
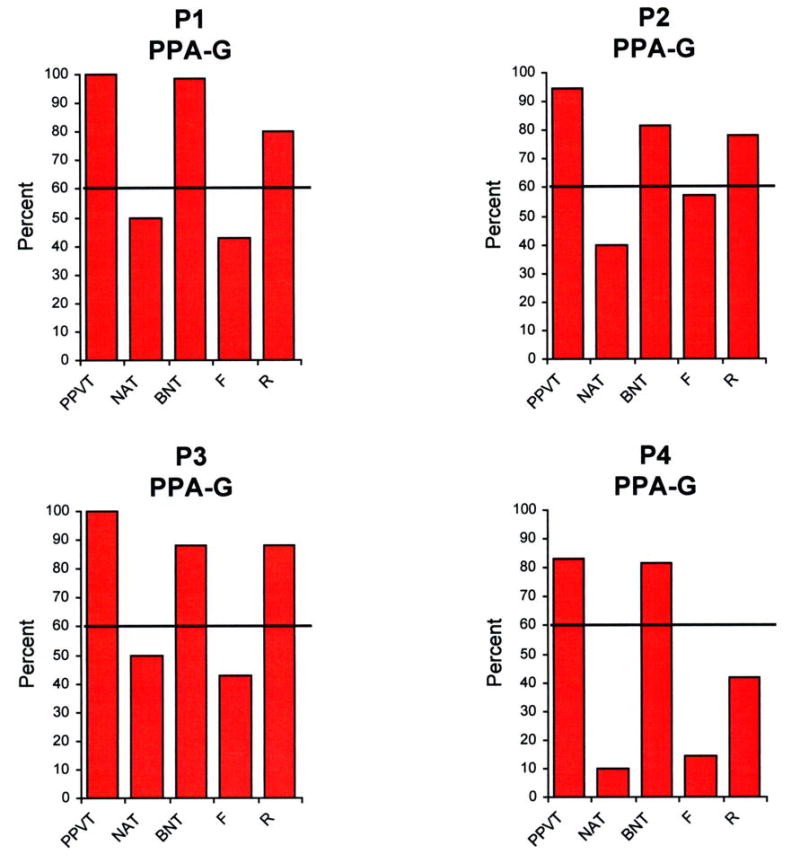
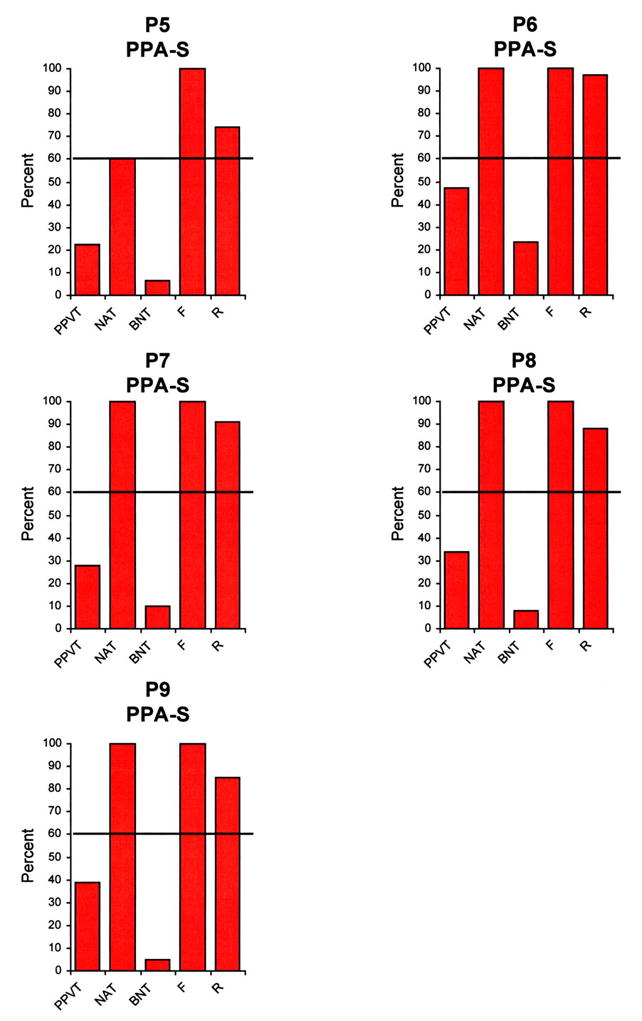
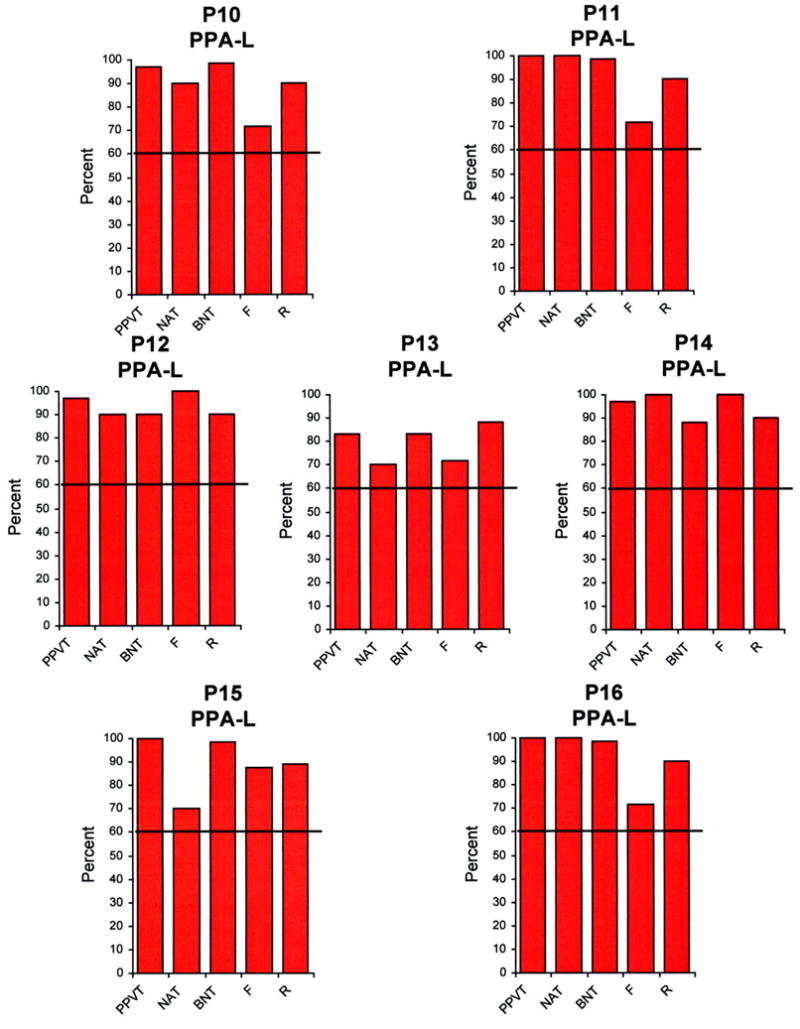
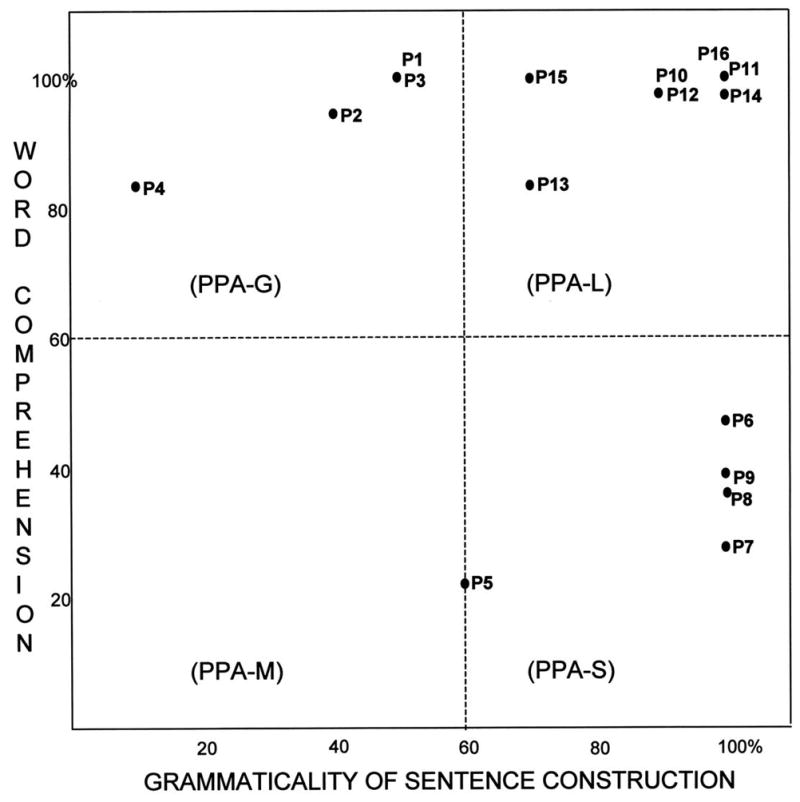
Objective: To provide a quantitative algorithm for classifying PPA into agrammatic (PPA-G), semantic (PPA-S), and logopenic (PPA-L) variants, each of which is known to have a different probability of association with Alzheimer disease vs frontotemporal lobar degeneration.
Design: Prospective study.
Setting: University medical center.
Patients: Sixteen consecutively enrolled patients with PPA who underwent neuropsychological testing and magnetic resonance imaging recruited nationally in the United States as part of a longitudinal study.
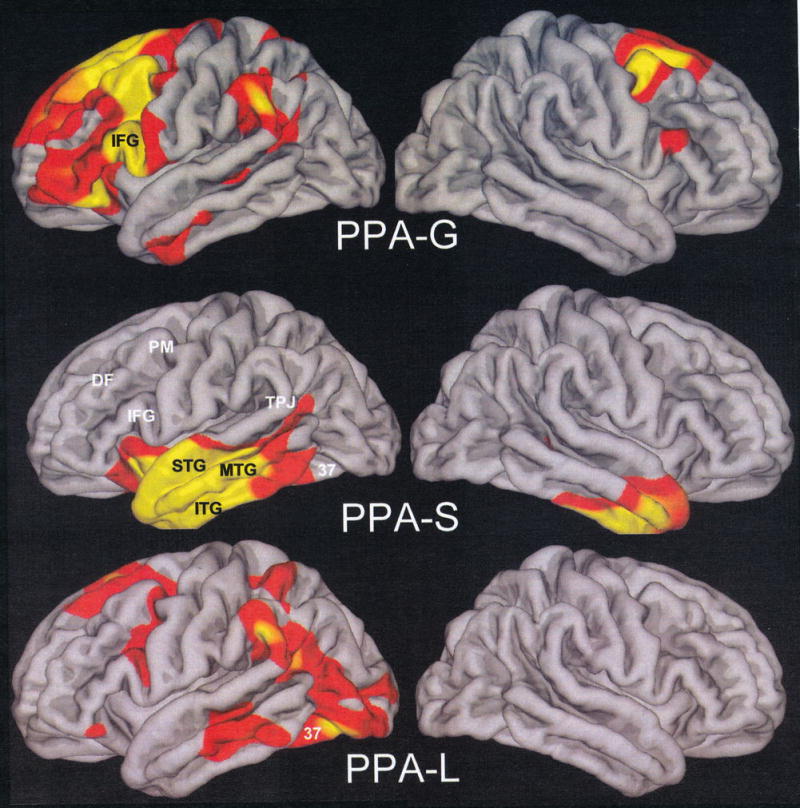
Results: A 2-dimensional template that reflects performance on tests of syntax (Northwestern Anagram Test) and lexical semantics (Peabody Picture Vocabulary Test-Fourth Edition) classified all 16 patients in concordance with a clinical diagnosis that had been made before the administration of quantitative tests. All 3 PPA subtypes had distinctly asymmetrical atrophy of the left perisylvian language network. Each subtype also had distinctive peak atrophy sites: PPA-G in the inferior frontal gyrus (Broca area), PPA-S in the anterior temporal lobe, and PPA-L in Brodmann area 37.
Conclusions: Once an accurate root diagnosis of PPA is made, subtyping can be quantitatively guided using a 2-dimensional template based on orthogonal tasks of grammatical competence and word comprehension. Although the choice of tasks and the precise cutoff levels may need to be adjusted to fit linguistic and educational backgrounds, these 16 patients demonstrate the feasibility of using a simple algorithm for clinicoanatomical classification in PPA. Prospective studies will show whether this subtyping can improve clinical prediction of the underlying neuropathologic condition.
Figures
References
-
- Knibb JA, Xuereb JH, Patterson K, Hodges JR. Clinical and pathological characterization of progressive aphasia. Annals of Neurology. 2006;59:156–165. - PubMed
-
- Mesulam M–M, Weintraub S. Primary progressive aphasia and kindred disorders. In: Duyckaerts C, Litvan I, editors. Handbook of Clinical Neurology. New York: Elsevier; 2008. pp. 573–587. - PubMed
-
- Mesulam M-M. Primary progressive aphasia: A language-based dementia. New England Journal of Medicine. 2003;348:1535–1542. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
