

A comparison of prediction models for fractures in older women: is more better?
- PMID: 20008691
- PMCID: PMC2811407
- DOI: 10.1001/archinternmed.2009.404
A comparison of prediction models for fractures in older women: is more better?
Abstract
Background: A Web-based risk assessment tool (FRAX) using clinical risk factors with and without femoral neck bone mineral density (BMD) has been incorporated into clinical guidelines regarding treatment to prevent fractures. However, it is uncertain whether prediction with FRAX models is superior to that based on parsimonious models.
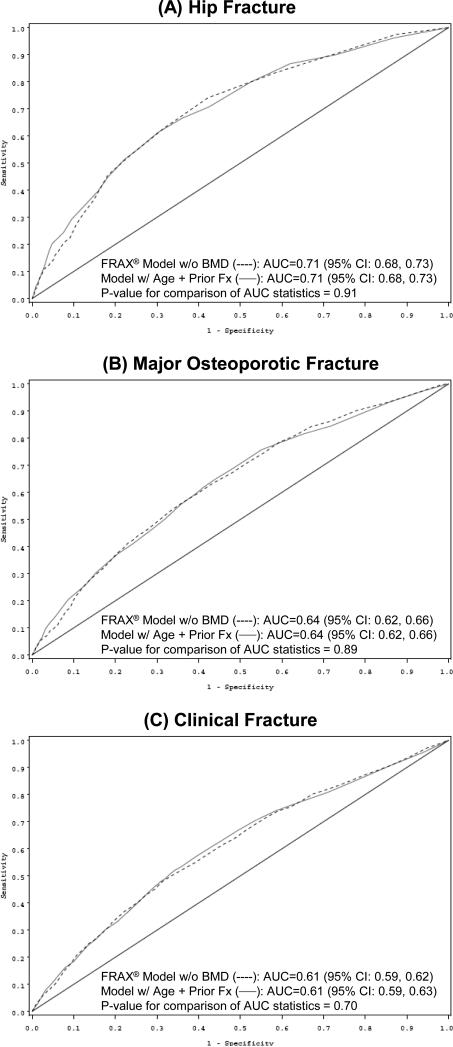
Methods: We conducted a prospective cohort study in 6252 women 65 years or older to compare the value of FRAX models that include BMD with that of parsimonious models based on age and BMD alone for prediction of fractures. We also compared FRAX models without BMD with simple models based on age and fracture history alone. Fractures (hip, major osteoporotic [hip, clinical vertebral, wrist, or humerus], and any clinical fracture) were ascertained during 10 years of follow-up. Area under the curve (AUC) statistics from receiver operating characteristic curve analysis were compared between FRAX models and simple models.
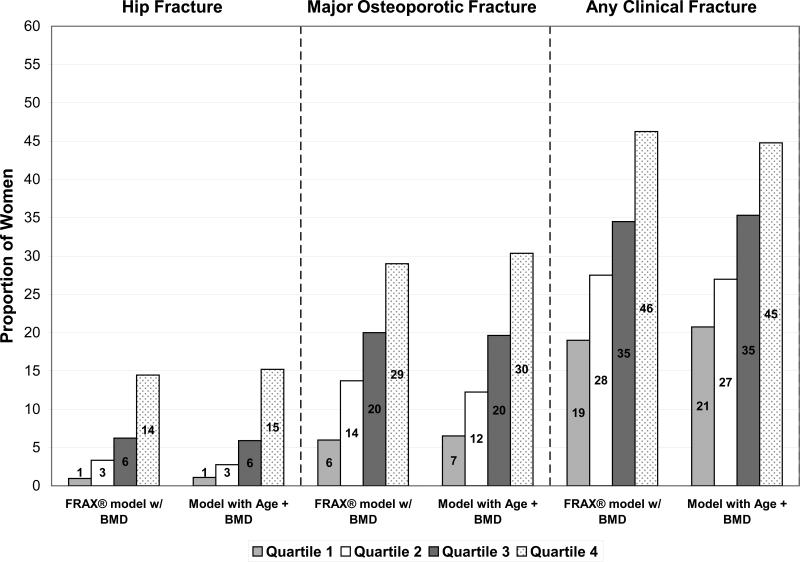
Results: The AUC comparisons showed no differences between FRAX models with BMD and simple models with age and BMD alone in discriminating hip (AUC, 0.75 for the FRAX model and 0.76 for the simple model; P = .26), major osteoporotic (AUC, 0.68 for the FRAX model and 0.69 for the simple model; P = .51), and clinical fracture (AUC, 0.64 for the FRAX model and 0.63 for the simple model; P = .16). Similarly, performance of parsimonious models containing age and fracture history alone was nearly identical to that of FRAX models without BMD. The proportion of women in each quartile of predicted risk who actually experienced a fracture outcome did not differ between FRAX and simple models (P > or = .16).
Conclusion: Simple models based on age and BMD alone or age and fracture history alone predicted 10-year risk of hip, major osteoporotic, and clinical fracture as well as more complex FRAX models.
Figures


Comment in
-
Should there be a fracas over FRAX and other fracture prediction tools?: Comment on "A comparison of prediction models for fractures in older women".Arch Intern Med. 2009 Dec 14;169(22):2094-5. doi: 10.1001/archinternmed.2009.2094. Arch Intern Med. 2009. PMID: 20008692 Free PMC article. No abstract available.
-
ACP Journal Club. Simple models predicted 10-year fracture risk in older women as accurately as more complex FRAX models.Ann Intern Med. 2010 Mar 16;152(6):JC3-13. doi: 10.7326/0003-4819-152-6-201003160-02013. Ann Intern Med. 2010. PMID: 20231555 No abstract available.
-
[Assessment of osteoporotic fracture risk: FRAX is exactly as inadequate as simple models].Praxis (Bern 1994). 2011 Apr 27;100(9):559-60. doi: 10.1024/1661-8157/a000522. Praxis (Bern 1994). 2011. PMID: 21526476 German. No abstract available.
References
-
- Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359:1761–1767. - PubMed
-
- Taylor BC, Schreiner PJ, Stone KL, et al. Long-term prediction of incident hip fracture risk in elderly white women: study of osteoporotic fractures. J Am Geriatr Soc. 2004;52:1479–1486. - PubMed
-
- Kanis JA. Diagnosis of osteoporosis and assessment of fracture risk. Lancet. 2002;359:1929–1936. - PubMed
-
- Kanis JA, Johansson H, Oden A, et al. A meta-analysis of prior corticosteroid use and fracture risk. J Bone Miner Res. 2004;19:893–899. - PubMed
Publication types
MeSH terms
Grants and funding
- AG05407/AG/NIA NIH HHS/United States
- R01 AR035583/AR/NIAMS NIH HHS/United States
- R01 AR035584/AR/NIAMS NIH HHS/United States
- AG05394/AG/NIA NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- AR35583/AR/NIAMS NIH HHS/United States
- AG005407/AG/NIA NIH HHS/United States
- R01 AG005394/AG/NIA NIH HHS/United States
- AR35584/AR/NIAMS NIH HHS/United States
- R01 AG027574/AG/NIA NIH HHS/United States
- AR35582/AR/NIAMS NIH HHS/United States
- AG027574/AG/NIA NIH HHS/United States
- AG027576/AG/NIA NIH HHS/United States
- R01 AG027576/AG/NIA NIH HHS/United States
- R01 AR035582/AR/NIAMS NIH HHS/United States
- AG005394/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
