

Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women's Health Initiative study
- PMID: 20008698
- PMCID: PMC10204121
- DOI: 10.1001/archinternmed.2009.436
Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women's Health Initiative study
Abstract
Background: Antidepressants are commonly prescribed medications, but their effect on cardiovascular morbidity and mortality remains unclear.
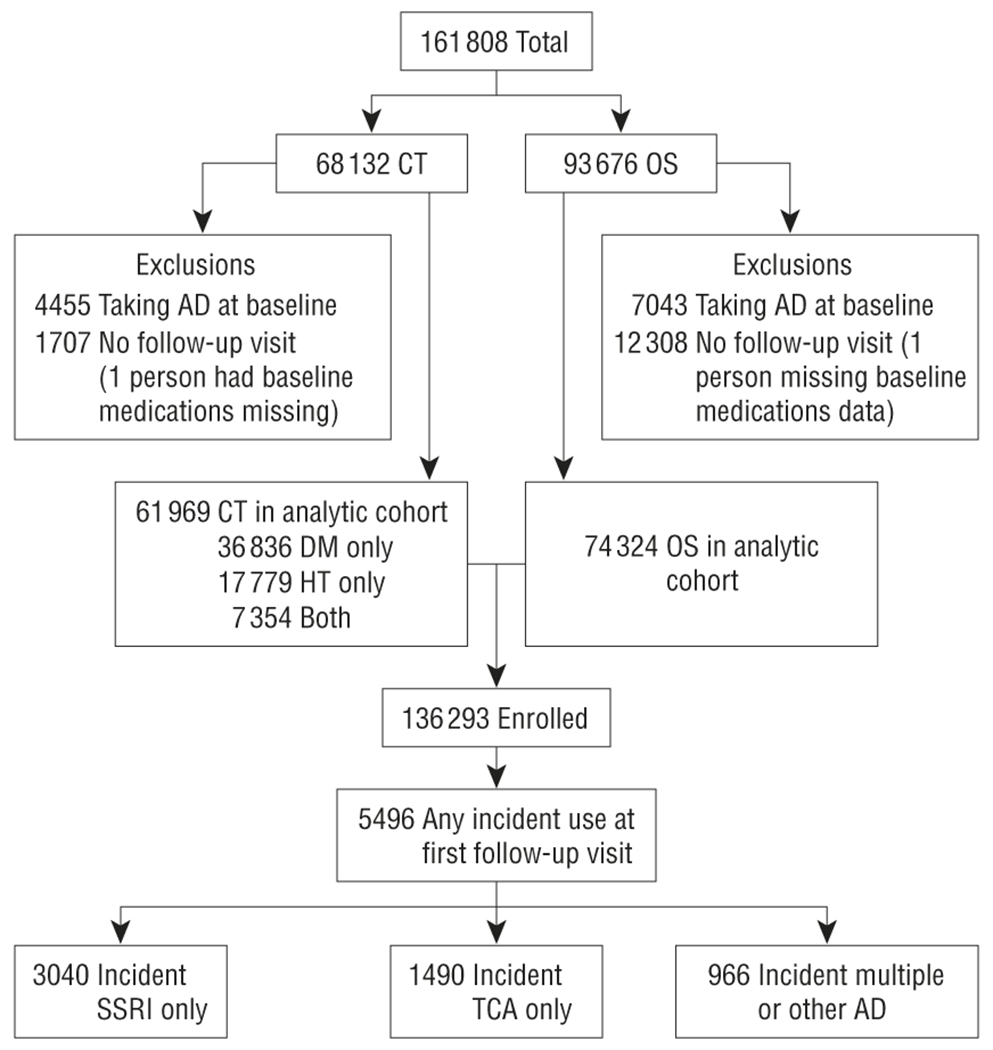
Methods: Prospective cohort study of 136 293 community-dwelling postmenopausal women in the Women's Health Initiative (WHI). Women taking no antidepressants at study entry and who had at least 1 follow-up visit were included. Cardiovascular morbidity and all-cause mortality for women with new antidepressant use at follow-up (n = 5496) were compared with those characteristics for women taking no antidepressants at follow-up (mean follow-up, 5.9 years).
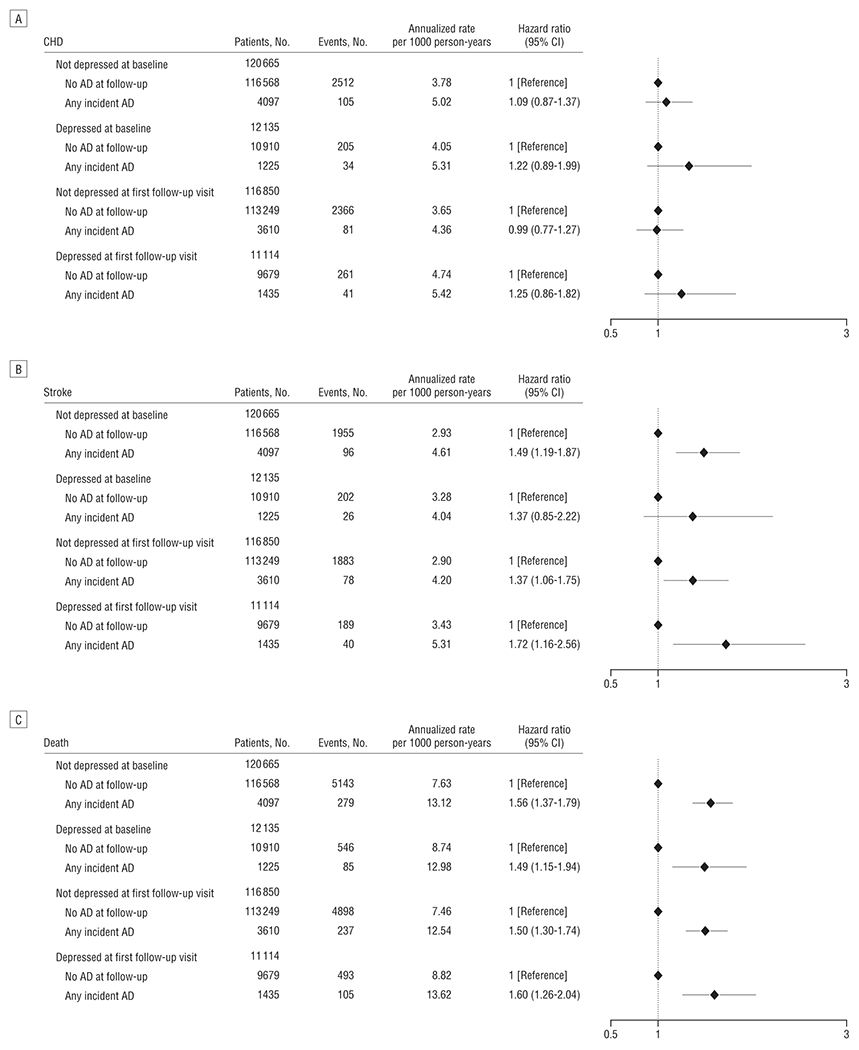
Results: Antidepressant use was not associated with coronary heart disease (CHD). Selective serotonin reuptake inhibitor (SSRI) use was associated with increased stroke risk (hazard ratio [HR],1.45, [95% CI, 1.08-1.97]) and all-cause mortality (HR,1.32 [95% CI, 1.10-1.59]). Annualized rates per 1000 person-years of stroke with no antidepressant use and SSRI use were 2.99 and 4.16, respectively, and death rates were 7.79 and 12.77. Tricyclic antidepressant (TCA) use was associated with increased risk of all-cause mortality (HR,1.67 [95% CI, 1.33-2.09]; annualized rate, 14.14 deaths per 1000 person-years). There were no significant differences between SSRI and TCA use in risk of any outcomes. In analyses by stroke type, SSRI use was associated with incident hemorrhagic stroke (HR, 2.12 [95% CI, 1.10-4.07]) and fatal stroke (HR, 2.10 [95% CI, 1.15-3.81]).
Conclusions: In postmenopausal women, there were no significant differences between SSRI and TCA use in risk of CHD, stroke, or mortality. Antidepressants were not associated with risk of CHD. Tricyclic antidepressants and SSRIs may be associated with increased risk of mortality, and SSRIs with increased risk of hemorrhagic and fatal stroke, although absolute event risks are low. These findings must be weighed against quality of life and established risks of cardiovascular disease and mortality associated with untreated depression.
Figures
Comment in
-
Antidepressant Use, Depression, and Poor Cardiovascular Outcomes: The Chicken or the Egg?: Comment on "Antidepressant Use and Risk of Incident Cardiovascular Morbidity and Mortality Among Postmenopausal Women in the Women's Health Initiative Study".Arch Intern Med. 2009 Dec 14;169(22):2140-1. doi: 10.1001/archinternmed.2009.437. Arch Intern Med. 2009. PMID: 20008699 No abstract available.
References
-
- Mojtabai R Increase in antidepressant medication in the US adult population between 1990 and 2003. Psychother Psychosom. 2008;77(2):83–92. - PubMed
-
- Montagnier D, Barberger-Gateau P, Jacqmin-Gadda H, et al. Evolution of prevalence of depressive symptoms and antidepressant use between 1988 and 1999 in a large sample of older French people: results from the personnes agées quid study. J Am Geriatr Soc. 2006;54(12):1839–1845. - PubMed
-
- Lett HS, Blumenthal JA, Babyak MA, et al. Depression as a risk factor for coronary artery disease: evidence, mechanisms, and treatment. Psychosom Med. 2004;66(3):305–315. - PubMed
-
- Salaycik KJ, Kelly-Hayes M, Beiser A, et al. Depressive symptoms and risk of stroke: the Framingham Study. Stroke. 2007;38(1):16–21. - PubMed
-
- Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women: the Women’s Health Initiative (WHI). Arch Intern Med. 2004;164(3):289–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
