

Epidemiology of the origins of airflow limitation in asthma
- PMID: 20008881
- PMCID: PMC2797072
- DOI: 10.1513/pats.200908-085DP
Epidemiology of the origins of airflow limitation in asthma
Abstract
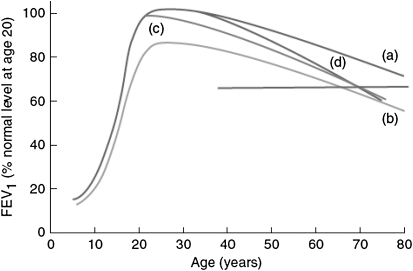
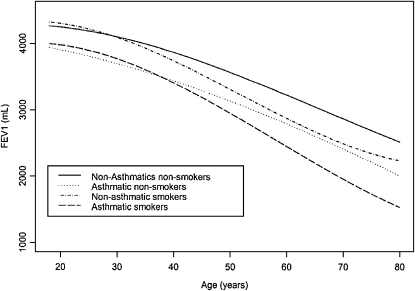
There is now conclusive evidence that, as a group, subjects with asthma have lower levels of lung function as compared with their peers and that a significant proportion of subjects with persistent asthma are at risk of developing non-fully reversible airflow limitation, the clinical hallmark of chronic obstructive pulmonary disease. Although at the population level the most conspicuous form of airflow limitation in asthma seems to be that of subjects who wheeze during the first years of life and whose symptoms persist into adult life, asthma-related lung deficits can be related to both acquired deficits in growth of lung function in childhood and steeper decline of lung function in adult life. These trajectories of lung function are likely to differ across subgroups of individuals with asthma, suggesting that different windows of opportunity may exist to modify the natural course of the disease before irreversible deficits are established. These observations indicate the importance of identifying biomarkers that can be used to target children and adults with asthma at increased risk for airflow limitation and determining whether pharmacological interventions can protect these patients from the development of chronic obstructive pulmonary disease.
Figures
References
-
- Ulrik CS, Backer V. Nonreversible airflow obstruction in life-long nonsmokers with moderate to severe asthma. Eur Respir J 1999;14:892–896. - PubMed
-
- van Rensen EL, Sont JK, Evertse CE, Willems LN, Mauad T, Hiemstra PS, Sterk PJ. Bronchial CD8 cell infiltrate and lung function decline in asthma. Am J Respir Crit Care Med 2005;172:837–841. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical