

Spatial heterogeneity of lung perfusion assessed with (13)N PET as a vascular biomarker in chronic obstructive pulmonary disease
- PMID: 20008987
- PMCID: PMC6698138
- DOI: 10.2967/jnumed.109.065185
Spatial heterogeneity of lung perfusion assessed with (13)N PET as a vascular biomarker in chronic obstructive pulmonary disease
Abstract
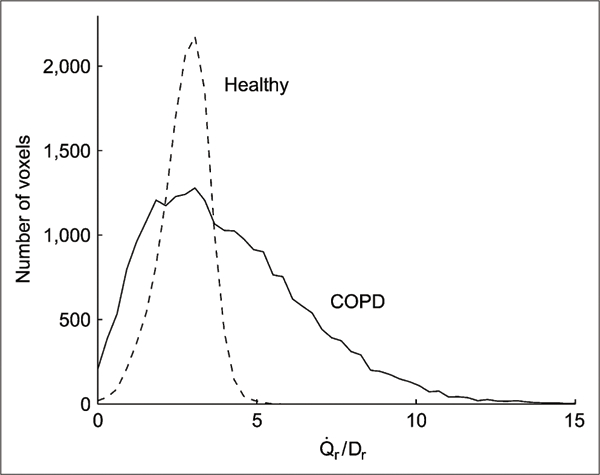
Although it is known that structural and functional changes in the pulmonary vasculature and parenchyma occur in the progress of chronic obstructive pulmonary disease (COPD), information is limited on early regional perfusion (Q(r)) alterations.
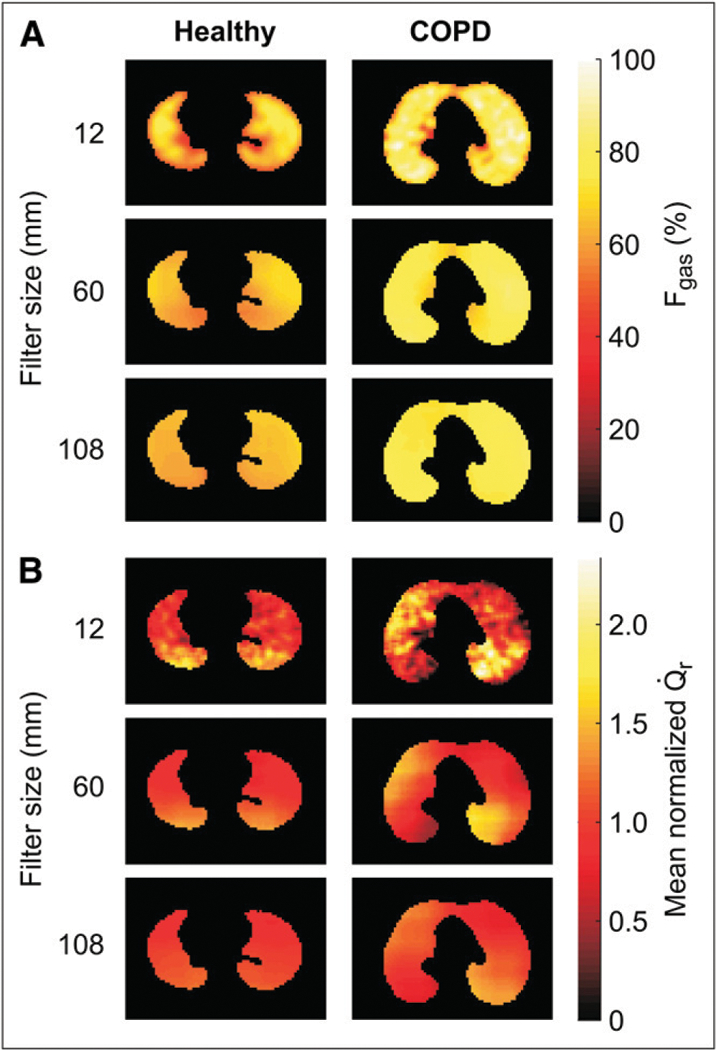
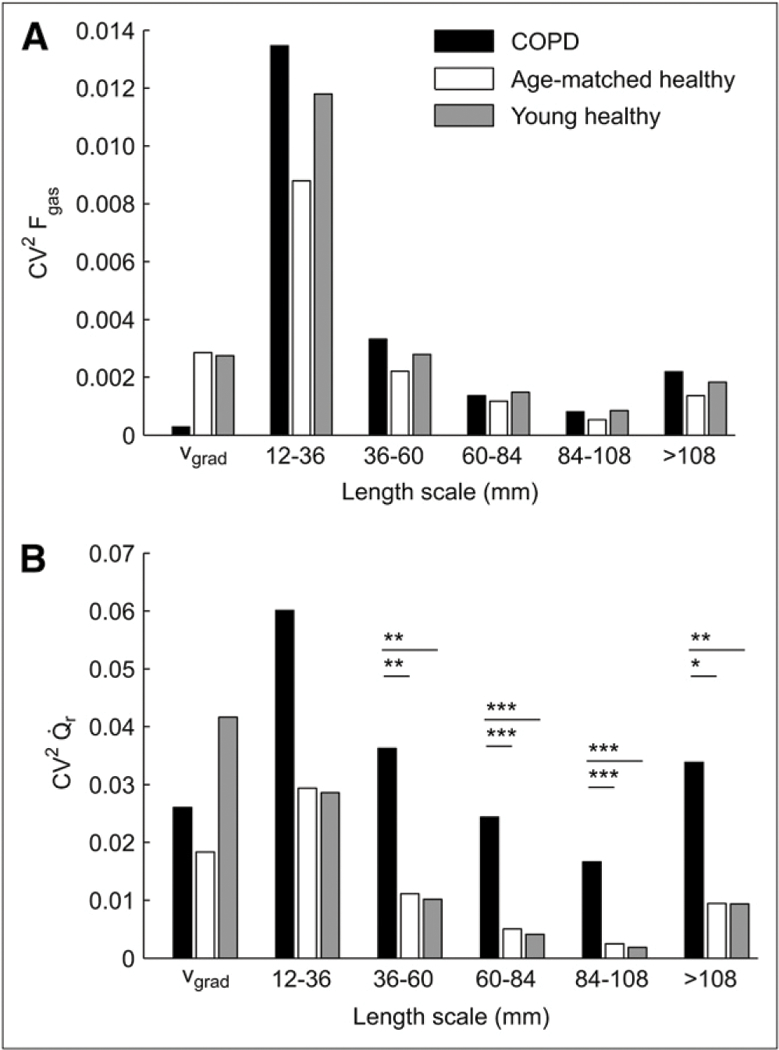
Methods: We studied 6 patients with mild or moderate COPD and 9 healthy subjects (6 young and 3 age-matched). The PET (13)NN-labeled saline injection method was used to compute images of Q(r) and regional ventilation (V(r)). Transmission scans were used to assess regional density. We used the squared coefficient of variation to quantify Q(r) heterogeneity and length-scale analysis to quantify the contribution to total perfusion heterogeneity of regions ranging from less than 12 to more than 108 mm.
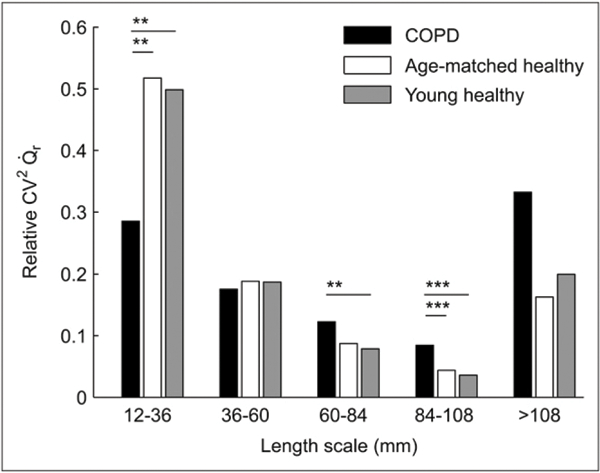
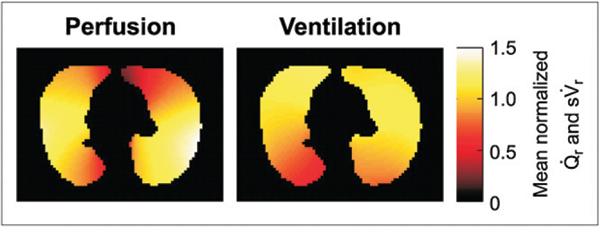
Results: Perfusion distribution in COPD subjects showed larger Q(r) heterogeneity, higher contribution from large length scales and lower contribution from small length scales, and larger heterogeneity of Q(r) normalized by tissue density than did healthy subjects. Dorsoventral gradients of V(r) were present in healthy subjects, with larger ventilation in dependent regions, whereas no gradient was present in COPD. Heterogeneity of ventilation-perfusion ratios was larger in COPD.
Conclusion: Q(r) is significantly redistributed in COPD. Q(r) heterogeneity in COPD patients is greater than in healthy subjects, mainly because of the contribution of large lung regions and not because of changes in tissue density or V(r). The assessment of spatial heterogeneity of lung perfusion with (13)NN-saline PET may serve as a vascular biomarker in COPD.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical