

Do hospitals provide lower quality of care to black patients for pneumonia?
- PMID: 20009756
- PMCID: PMC3774066
- DOI: 10.1097/CCM.0b013e3181c8fd58
Do hospitals provide lower quality of care to black patients for pneumonia?
Abstract
Objectives: Recent studies reported lower quality of care for black vs. white patients with community-acquired pneumonia and suggested that disparities persist at the individual hospital level. We examined racial differences in emergency department and intensive care unit care processes to determine whether differences persist after adjusting for case-mix and variation in care across hospitals.
Design: Prospective, observational cohort study.
Setting: Twenty-eight U.S. hospitals.
Patients: Patients with community-acquired pneumonia: 1738 white and 352 black patients.
Interventions: None.
Measurements: We compared care quality based on antibiotic receipt within 4 hrs and adherence to American Thoracic Society antibiotic guidelines, and intensity based on intensive care unit admission and mechanical ventilation use. Using random effects and generalized estimating equations models, we adjusted for case-mix and clustering of racial groups within hospitals and estimated odds ratios for differences in care within and across hospitals.
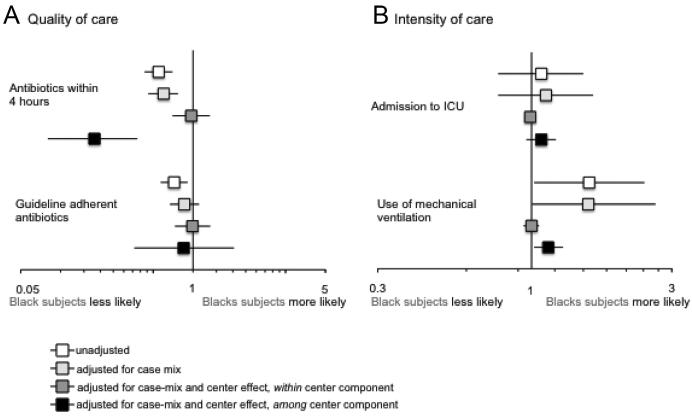
Main results: Black patients were less likely to receive antibiotics within 4 hrs (odds ratio, 0.55; 95% confidence interval, 0.43-0.70; p < .001) and less likely to receive guideline-adherent antibiotics (odds ratio, 0.72; 95% confidence interval, 0.57-0.91; p = .006). These differences were attenuated after adjusting for casemix (odds ratio, 0.59; 95% confidence interval; 0.46-0.76 and 0.84; 95% confidence interval, 0.66 -1.09). Within hospitals, black and white patients received similar care quality (odds ratio, 1; 95% confidence interval, 0.97-1.04 and 1; 95% confidence interval, 0.97-1.03). However, hospitals that served a greater proportion of black patients were less likely to provide timely antibiotics (odds ratio, 0.84; 95% confidence interval, 0.78-0.90). Black patients were more likely to receive mechanical ventilation (odds ratio, 1.57; 95% confidence interval, 1.02-2.42; p = .042). Again, within hospitals, black and white subjects were equally likely to receive mechanical ventilation (odds ratio, 1; 95% confidence interval, .94-1.06) and hospitals that served a greater proportion of black patients were more likely to institute mechanical ventilation (odds ratio, 1.13; 95% confidence interval, 1.02-1.25).
Conclusions: Black patients appear to receive lower quality and higher intensity of care in crude analyses. However, these differences were explained by different case-mix and variation in care across hospitals. Within the same hospital, no racial differences in care were observed.
Figures
Comment in
-
Deconstructing racial and ethnic disparities in critical care.Crit Care Med. 2010 Mar;38(3):978-80. doi: 10.1097/CCM.0b013e3181cc15d3. Crit Care Med. 2010. PMID: 20168151 No abstract available.
References
-
- Ayanian JZ, Weissman JS, Chasan-Taber S, et al. Quality of care by race and gender for congestive heart failure and pneumonia. Med Care. 1999;37:1260–1269. - PubMed
-
- Jha AK, Orav EJ, Li Z, et al. Concentration and quality of hospitals that care for elderly black patients. Arch Intern Med. 2007;167:1177–1182. - PubMed
-
- Hasnain-Wynia R, Baker DW, Nerenz D, et al. Disparities in health care are driven by where minority patients seek care: Examination of the hospital quality alliance measures. Arch Intern Med. 2007;167:1233–1239. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
