

Early clinical and programmatic outcomes with tenofovir-based antiretroviral therapy in Zambia
- PMID: 20009765
- PMCID: PMC2862003
- DOI: 10.1097/QAI.0b013e3181c6c65c
Early clinical and programmatic outcomes with tenofovir-based antiretroviral therapy in Zambia
Abstract
Background: In July 2007, amid some controversy over cost, Zambia was the first African country to introduce tenofovir (TDF) as a component of first-line antiretroviral therapy (ART) on a wide scale.
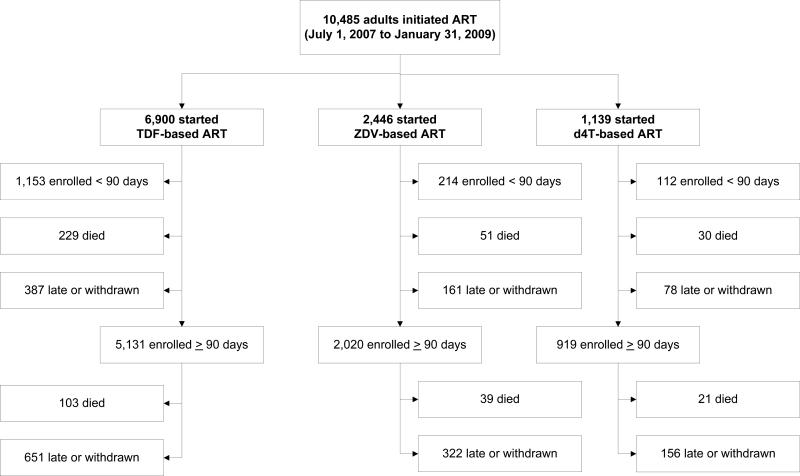
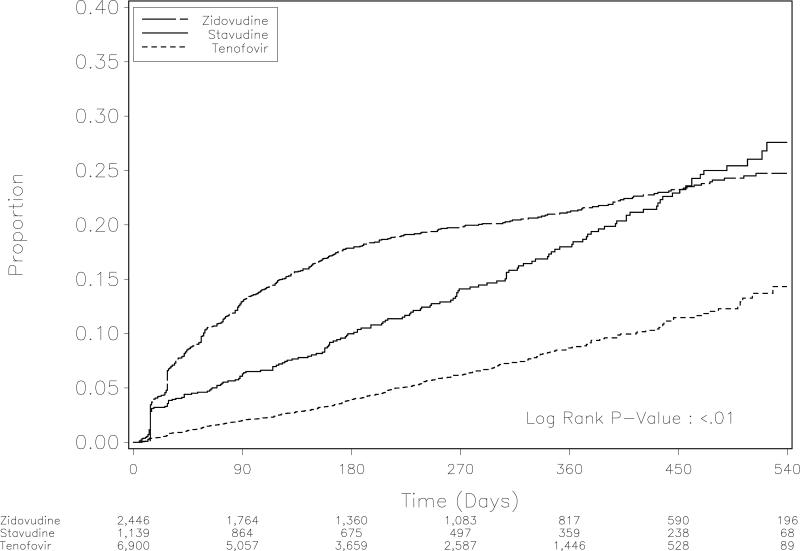
Methods: We compared drug substitutions, mortality, and "programmatic failure" among adults starting TDF-, zidovudine (ZDV)-, and stavudine (d4T)-containing ART. Programmatic failure was defined as death, withdrawal, or loss to follow-up.
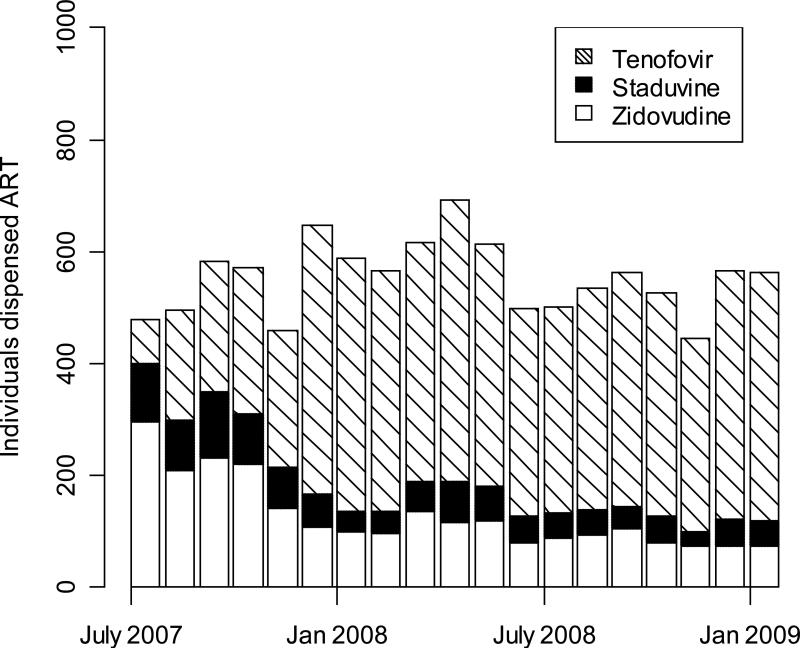
Results: Between July 2007 and January 2009, 10,485 adults initiated ART (66% on TDF, 23% on ZDV, 11% on d4T), with a median follow-up time of 239 (interquartile range 98, 385) days. Those starting TDF were more likely to be male and more likely to have indicators of severe disease at baseline. In adjusted Cox proportional hazards models, ZDV- (adjusted hazard ratio [AHR] = 2.74, 95% confidence interval [CI] = 2.30-3.28) and d4T-based regimens (AHR = 1.92, 95% CI = 1.55-2.38) were associated with higher risk for drug substitution when compared with TDF-based regimens. Similar hazards were noted for overall mortality (ZDV: AHR = 0 .81, 95% CI = 0.62-1.06; d4T: AHR = 1.03, 95% CI = 0.74-1.43) and programmatic failure (ZDV: AHR = 0.99, 95% CI = 0.88-1.11; d4T: AHR = 1.11, 95% CI = 0.96-1.28) when compared with TDF.
Conclusions: TDF is associated with similar clinical and programmatic outcomes as ZDV and d4T but appears to be better tolerated. Although further evaluation is needed, these results are encouraging and support Zambia's policy decision.
Figures


References
-
- Gallant JE, Staszewski S, Pozniak AL, et al. Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral-naive patients: a 3-year randomized trial. JAMA. 2004 Jul 14;292(2):191–201. - PubMed
-
- Gallant JE, DeJesus E, Arribas JR, et al. Tenofovir DF, emtricitabine, and efavirenz vs. zidovudine, lamivudine, and efavirenz for HIV. N Engl J Med. 2006 Jan 19;354(3):251–260. - PubMed
-
- DART Virology Group and Trial Team Virological response to a triple nucleoside/nucleotide analogue regimen over 48 weeks in HIV-1-infected adults in Africa. AIDS. 2006 Jun 26;20(10):1391–1399. - PubMed
-
- Medecins Sans Frontieres Untangling the web of antiretroviral price reductions: 11th edition. [March 2, 2009]. http://www.msfaccess.org.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
