

Effectiveness of an aspiration risk-reduction protocol
- PMID: 20010041
- PMCID: PMC2875939
- DOI: 10.1097/NNR.0b013e3181c3ba05
Effectiveness of an aspiration risk-reduction protocol
Abstract
Background: Aspiration of gastric contents is a serious problem in critically ill, mechanically ventilated patients receiving tube feedings.
Objectives: The purpose of this study was to evaluate the effectiveness of a three-pronged intervention to reduce aspiration risk in a group of critically ill, mechanically ventilated patients receiving tube feedings.
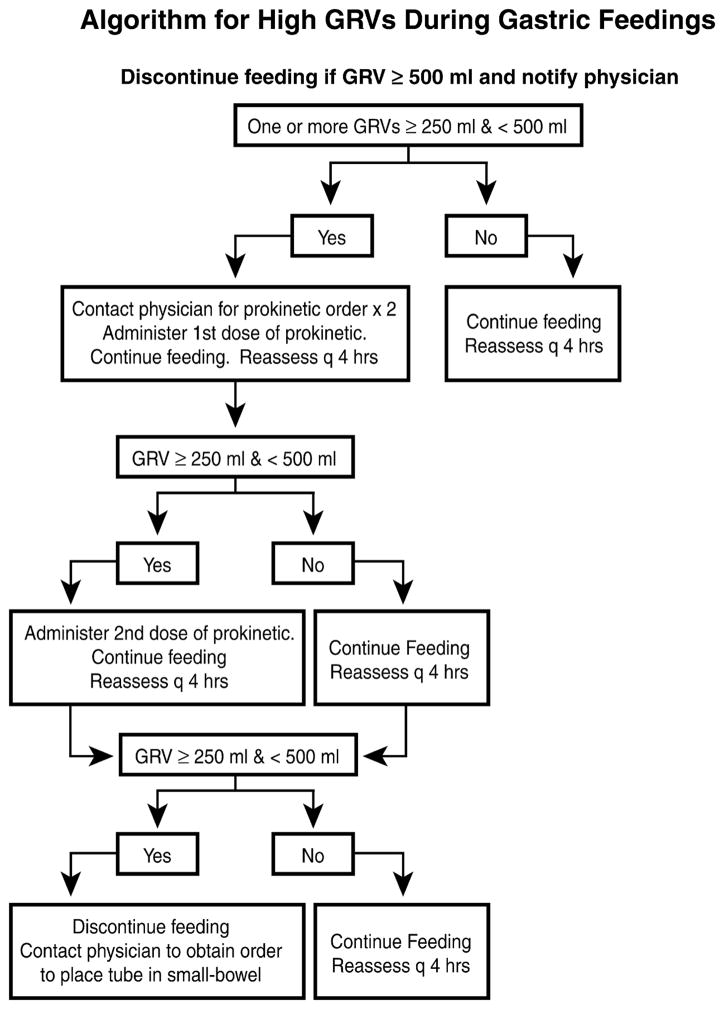
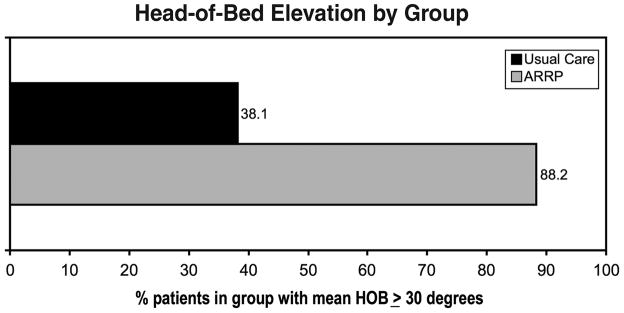
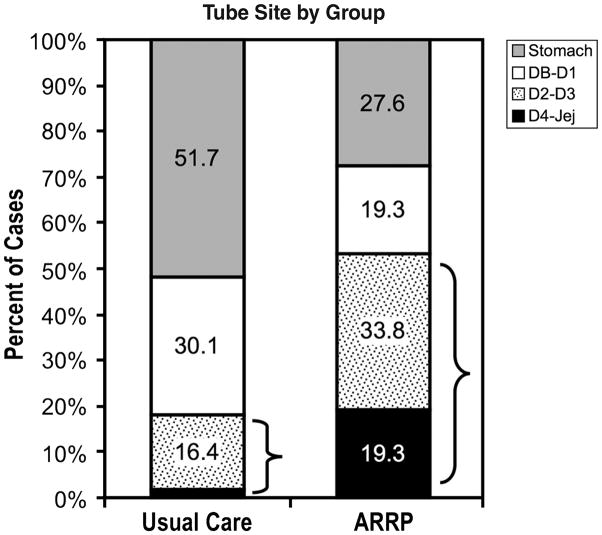
Methods: A two-group quasi-experimental design was used to compare outcomes of a usual care group (December 2002-September 2004) with those of an Aspiration Risk-Reduction Protocol (ARRP) group (January 2007-April 2008). The incidence of aspiration and pneumonia was compared between the usual care group (n = 329) and the ARRP group (n = 145). The ARRP had three components: maintaining head-of-bed elevation at 30 degrees or higher, unless contraindicated; inserting feeding tubes into distal small bowel, when indicated; and using an algorithmic approach for high gastric residual volumes.
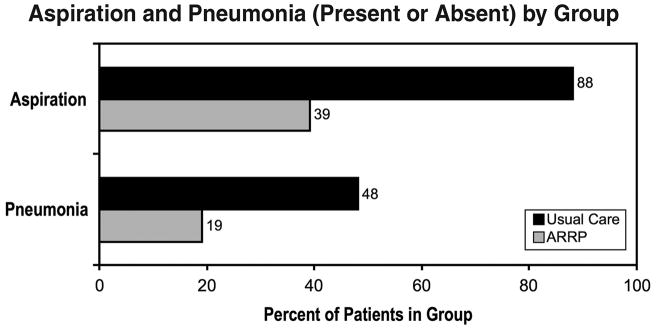
Results: Two of the three ARRP components were implemented successfully. Almost 90% of the ARRP group had mean head-of-bed elevations of 30 degrees or higher as compared to 38% in the usual care group. Almost three fourths of the ARRP group had feeding tubes placed in the small bowel as compared with less than 50% in the usual care group. Only three patients met the criteria for the high gastric residual volume algorithm. Aspiration was much lower in the ARRP group than that in the usual care group (39% vs. 88%, respectively). Similarly, pneumonia was much lower in the ARRP group than that in the usual care group (19% vs. 48%, respectively).
Discussion: Findings from this study suggest that a combination of a head-of-bed position elevated to at least 30 degrees and use of a small-bowel feeding site can reduce the incidence of aspiration and aspiration-related pneumonia dramatically in critically ill, tube-fed patients.
Figures
References
-
- Booth CM, Heyland DK, Paterson WG. Gastrointestinal promotility drugs in the critical care setting: A systematic review of the evidence. Critical Care Medicine. 2002;30(7):1429–1435. - PubMed
-
- Bourgault AM, Ipe L, Weaver J, Swartz S, O’dea PJ. Development of evidence-based guidelines and critical care nurses’ knowledge of enteral feeding. Critical Care Nurse. 2007;27(4):17–22. 25–29. - PubMed
-
- Damiano AM, Bergner M, Draper EA, Knaus WA, Wagner DP. Reliability of a measure of severity of illness: Acute physiology of chronic health evaluation--II. Journal of Clinical Epidemiology. 1992;45(2):93–101. - PubMed
-
- de Lemos J, Tweeddale M, Chittock D. Measuring quality of sedation in adult mechanically ventilated critically ill patients. The Vancouver Interaction and Calmness Scale. Sedation Focus Group. Journal of Clinical Epidemiology. 2000;53(9):908–919. - PubMed
-
- Dubow JS, Leikin J, Rezak M. Acute chorea associated with metoclopramide use. American Journal of Therapeutics. 2006;13(6):543–544. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
