

Impact of pregnancy-induced hypertension on stillbirth and neonatal mortality
- PMID: 20010214
- PMCID: PMC2841017
- DOI: 10.1097/EDE.0b013e3181c297af
Impact of pregnancy-induced hypertension on stillbirth and neonatal mortality
Abstract
Background: Hypertensive disorders of pregnancy are more frequent in primiparous women, but may be more severe in multiparas. We examined trends in stillbirth and neonatal mortality related to pregnancy-induced hypertension (PIH), and explored whether mortality varied by parity and maternal race.
Methods: We carried out a population-based study of 57 million singleton live births and stillbirths (24-46 weeks' gestation) in the United States between 1990 and 2004. We estimated rates and adjusted odds ratios (ORs) of stillbirth and neonatal death in relation to PIH, comparing births in 1990-1991 with 2003-2004.
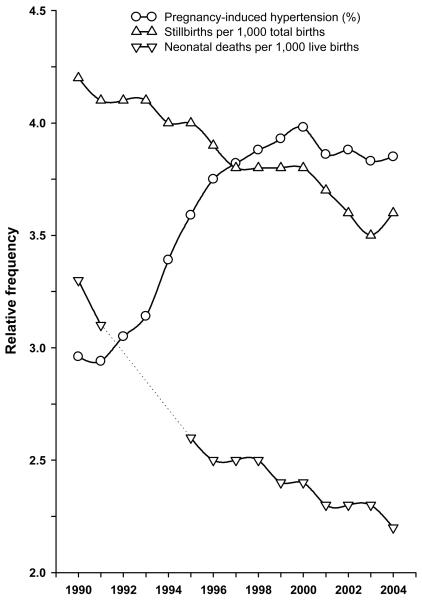
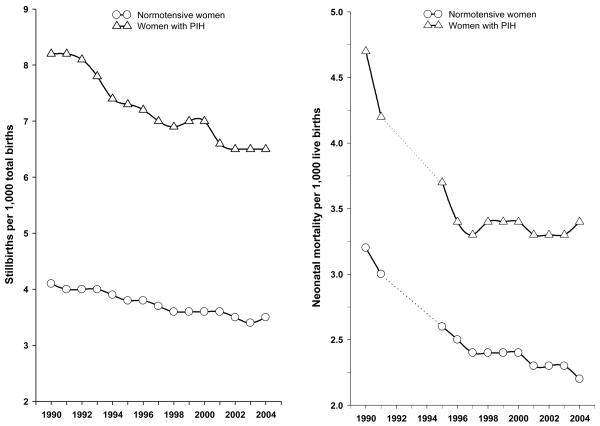
Results: PIH increased from 3.0% in 1990-1991 to 3.8% in 2003-2004. In both periods, PIH was associated with a higher risk of stillbirth and neonatal death. We explored this in more detail in 2003-2004, and observed that the increased risk of PIH-related stillbirth was higher in women having their second or higher-order births (OR = 2.2 [95% confidence interval = 2.1-2.4]) compared with women having their first birth (1.5 [1.4-1.6]). Patterns were similar for neonatal death (1.3 [1.2-1.4] in first and 1.6 [1.5-1.8] in second or higher-order births). Among multiparas, the association between PIH and stillbirth was stronger in black women (2.9 [2.7-3.2]) than white women (2.0 [1.8-2.1]).
Conclusions: A substantial burden of stillbirth and neonatal mortality is associated with PIH, especially among multiparous women, which may be due to more severe PIH, or to a higher burden of underlying disease.
Figures
References
-
- Ananth CV, Peedicayil A, Savitz DA. Effect of hypertensive diseases in pregnancy on birthweight, gestational duration, and small-for-gestational-age births. Epidemiology. 1995;6(4):391–5. - PubMed
-
- Xiao R, Sorensen TK, Williams MA, Luthy DA. Influence of pre-eclampsia on fetal growth. J Matern Fetal Neonatal Med. 2003;13(3):157–62. - PubMed
-
- Xiong X, Buekens P, Pridjian G, Fraser WD. Pregnancy-induced hypertension and perinatal mortality. J Reprod Med. 2007;52(5):402–6. - PubMed
-
- Zhang J, Meikle S, Trumble A. Severe maternal morbidity associated with hypertensive disorders in pregnancy in the United States. Hypertens Pregnancy. 2003;22(2):203–12. - PubMed
-
- Zhang J, Zeisler J, Hatch MC, Berkowitz G. Epidemiology of pregnancy-induced hypertension. Epidemiol Rev. 1997;19(2):218–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
