

Five-year outcomes of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y gastric bypass in a comprehensive bariatric surgery program in Canada
- PMID: 20011160
- PMCID: PMC2792387
Five-year outcomes of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y gastric bypass in a comprehensive bariatric surgery program in Canada
Abstract
Background: Bariatric surgery remains the most effective modality to induce sustainable weight loss in the morbidly obese. Our aim was to compare outcomes between the laparoscopic Roux-en-Y gastric bypass (LRYGBP) and the laparoscopic adjustable gastric banding device (LAGBD) method with 5-year follow-up in a Canadian bariatric surgery centre.
Methods: This is a retrospective outcomes analysis of 1035 laparoscopic bariatric procedures performed over 7 years. We extracted data from our prospectively collected bariatric surgery registry from Feb. 1, 2002, to Jun. 30, 2008. We evaluated patient demographics, weight loss, complications, mortality and need for revision surgery by procedure type.
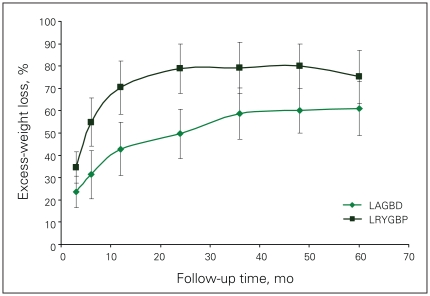
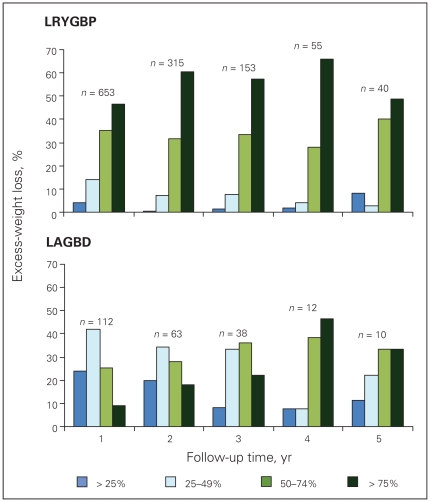
Results: We examined outcomes in 149 (14.4%) LAGBD and 886 (85.6%) LRYGBP procedures. The mean body mass index (BMI) was significantly higher in the LRYGBP group (50.9, standard deviation [SD] 8.9, v. 45.0, SD 6.7) whereas age and sex ratio were the same. There were 3 deaths (0.3%) in the LRYGBP group and no deaths in the LAGBD group. Sixteen patients (10.8%) in the LAGBD group needed conversion to LRYGBP because of poor weight loss, band intolerance, band erosion or slippage, and 6 patients (0.7%) in the LRYGBP group required revision because of inability to achieve the desired weight loss. The percent excess-weight loss was 41, 49, 59, 60 and 61 at 1, 2, 3, 4 and 5 years postsurgery for the LAGBD patients who kept their band, and 70, 79, 79, 79 and 75 for the LRYGBP patients.
Conclusion: Laparoscopic weight loss surgery can be performed safely with acceptable mortality. Our study suggests superior weight loss and low revision requirement for the LRYGBP, making this a more durable procedure in a publicly funded health care system.
Contexte: La chirurgie bariatrique demeure le moyen le plus efficace de provoquer une perte de poids durable chez les patients atteints d’obésité morbide. Nous voulions comparer les résultats du pontage gastrique Roux-en-Y par laparoscopie (PGRYL) à ceux de la méthode de l’anneau gastrique ajustable par laparoscopie (AGAL) avec un suivi sur 5 ans dans un centre canadien de chirurgie bariatrique.
Méthodes: Il s’agit d’une analyse rétrospective des résultats de 1035 interventions bariatriques par laparoscopie pratiquées en 7 ans. Nous avons extrait des données de notre registre prospectif de chirurgie bariatrique pour la période du 1 février 2002 au 30 juin 2008. Nous avons évalué les caractéristiques démographiques des patients, la perte de poids, les complications, la mortalité et le besoin d’une chirurgie de révision selon le type d’intervention.
Résultats: Nous avons analysé les résultats de 149 (14,4 %) interventions AGAL et 886 (85,6 %) interventions PGRYL. L’indice de masse corporelle (IMC) était beau-coup plus élevé chez les patients du groupe PGRYL (50,9, écart-type [ET] 8,9, c. 45,0, ET 6,7) tandis que les ratios d’âge et de sexe étaient les mêmes. Il y a eu 3 décès (0,3 %) chez les patients du groupe PGRYL et aucun chez ceux du groupe AGAL. Dans le groupe AGAL, 16 (10,8 %) des patients ont dû recevoir une conversion à la méthode PGRYL à cause de la faible perte de poids, de l’intolérance de l’anneau, de l’érosion ou du glissement de l’anneau, et dansle groupe PGRYL, 6 (0,7 %) patients ont eu besoin d’une révision parce qu’ils n’ont pu perdre autant de poids qu’ils le souhaitaient. Après 1, 2, 3, 4 et 5 ans suivant l’intervention chirurgicale, le pourcentage de perte de poids excédentaire s’est établi à 41, 49, 59, 60 et 61 chez ceux qui ont subi l’intervention AGAL et à 70, 79, 79, 79 et 75 chez les patients qui ont subi une intervention de type PGRYL.
Conclusion: L’intervention chirurgicale par laparoscopie pour perte de poids peut être pratiquée en toute sécurité avec un taux de mortalité acceptable. Notre étude indique que la méthode PGRYL fait perdre plus de poids et exige peu de révisions, ce qui en fait une intervention plus viable dans un système de santé public.
Figures
References
-
- Rapport du groupe d’experts en santé publique, médecine et chirurgie bariatrique avec la collaboration des agences de la santé de la capitale nationale, de la Mauricie-Centre-Du-Québec et Montréal. L’organisation de la médecine et chirurgie bariatriques au Québec. 2007;1:1.
-
- Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894(i–xii):1–253. - PubMed
-
- Abelson P, Kennedy D. The obesity epidemic. Science. 2004;304:1413. - PubMed
-
- Torrance GM, Hooper MD, Reeder BA. Trends in overweight and obesity among adults in Canada (1970–1992) evidence from national surveys using measured height and weight. Int J Obes Relat Metab Disord. 2002;26:797–804. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous