

Sphincter-sparing resection for rectal cancer
- PMID: 20011201
- PMCID: PMC2789515
- DOI: 10.1055/s-2007-984864
Sphincter-sparing resection for rectal cancer
Abstract
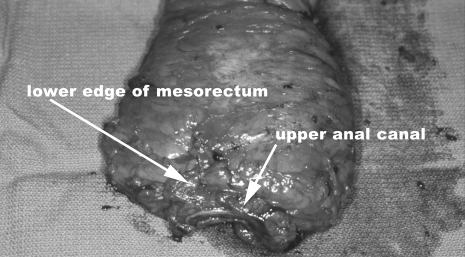
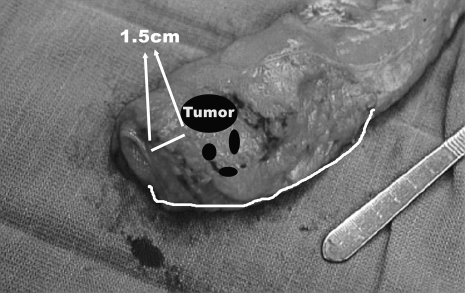
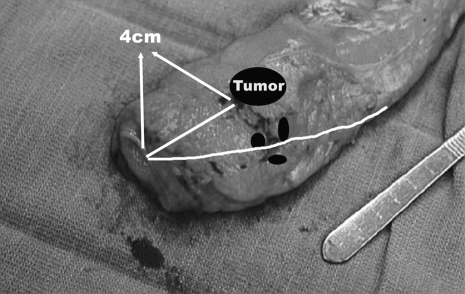
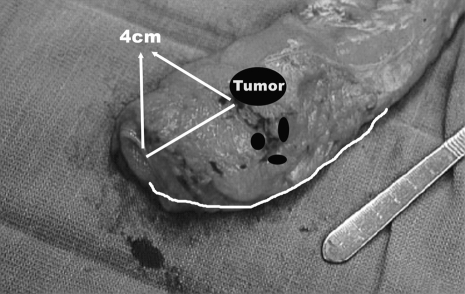
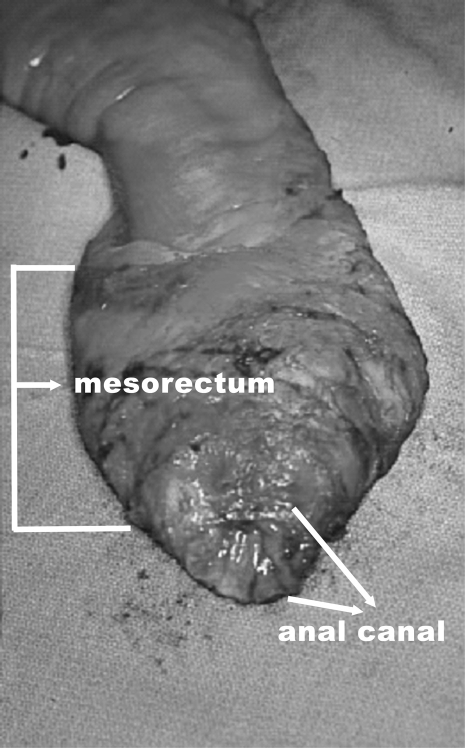
Although there is still a place for abdominoperineal resection in the treatment of rectal cancer, the state of the art is sphincter-preserving resection. Even for the lowest of rectal cancers, using a combination of neoadjuvant chemo/radiation, total mesorectal excision, and intersphincteric proctectomy and colonic J-pouch to anal anastomosis, sphincter preservation can be achieved for most patients. The key concept in pushing sphincter preservation forward has been the realization that the deep, circumferential, or lateral margin is all-important. Unless the rectal tumor involves the external sphincter muscle, there is no oncologic need to remove it, and following resection of the tumor, gastrointestinal tract continuity can be restored.
Keywords: Sphincter-preserving resection; coloanal anastomosis; intersphincteric resection; low anterior resection; total mesorectal excision.
Figures
Similar articles
-
Sphincter preservation in low rectal cancer is facilitated by preoperative chemoradiation and intersphincteric dissection.Ann Surg. 2009 Feb;249(2):236-42. doi: 10.1097/SLA.0b013e318195e17c. Ann Surg. 2009. PMID: 19212176
-
Laparoscopic intersphincteric resection for low rectal cancer.Surg Oncol. 2007 Dec;16 Suppl 1:S117-20. doi: 10.1016/j.suronc.2007.10.006. Epub 2007 Nov 26. Surg Oncol. 2007. PMID: 18023571
-
[Risk factors of coloanal anastomotic stricture after laparoscopic intersphincteric resection for low rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Aug 25;22(8):755-761. doi: 10.3760/cma.j.issn.1671-0274.2019.08.010. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31422614 Chinese.
-
[Colonic pouch and other procedures to improve the continence after low anterior rectal resection with TME].Zentralbl Chir. 2008 Apr;133(2):107-15. doi: 10.1055/s-2008-1004735. Zentralbl Chir. 2008. PMID: 18415896 Review. German.
-
Methods and results of sphincter-preserving surgery for rectal cancer.Cancer Control. 2003 May-Jun;10(3):212-8. doi: 10.1177/107327480301000304. Cancer Control. 2003. PMID: 12794619 Review.
Cited by
-
Bursectomy in gastric cancer surgery: surgical technique and operative safety.Updates Surg. 2013 Jun;65(2):95-101. doi: 10.1007/s13304-013-0210-7. Epub 2013 Apr 17. Updates Surg. 2013. PMID: 23592040
-
Shared Decision-Making, Sphincter Preservation, and Rectal Cancer Treatment: Identifying and Executing What Matters Most to Patients.Clin Colon Rectal Surg. 2023 Jul 19;37(4):256-265. doi: 10.1055/s-0043-1770720. eCollection 2024 Jul. Clin Colon Rectal Surg. 2023. PMID: 38882940 Free PMC article. Review.
-
Low rectal cancer: Sphincter preserving techniques-selection of patients, techniques and outcomes.World J Gastrointest Oncol. 2015 Jul 15;7(7):55-70. doi: 10.4251/wjgo.v7.i7.55. World J Gastrointest Oncol. 2015. PMID: 26191350 Free PMC article.
-
Multi-institutional assessment of sphincter preservation for rectal cancer.Ann Surg Oncol. 2014 Dec;21(13):4075-80. doi: 10.1245/s10434-014-3882-4. Epub 2014 Jul 8. Ann Surg Oncol. 2014. PMID: 25001097 Free PMC article.
-
Machine learning for prediction of chemoradiation therapy response in rectal cancer using pre-treatment and mid-radiation multi-parametric MRI.Magn Reson Imaging. 2019 Sep;61:33-40. doi: 10.1016/j.mri.2019.05.003. Epub 2019 May 3. Magn Reson Imaging. 2019. PMID: 31059768 Free PMC article.
References
-
- Jessup J M, Gunderson L L, Greene F L, et al. In: Greene FL, Page AL, Fleming ID, et al, editor. AJCC Cancer Staging Manual. 6th ed. New York, NY: Springer; 2002. Colon and rectum. pp. 113–124.
-
- Miles W E. Cancer of the Rectum. London: Harrison; 1926.
-
- Williams N S. The rationale for preservation of the anal sphincter in patients with low rectal cancer. Br J Surg. 1984;71:575–581. - PubMed
-
- Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–1740. - PubMed
