

Reoperative inflammatory bowel disease surgery
- PMID: 20011321
- PMCID: PMC2780117
- DOI: 10.1055/s-2006-956440
Reoperative inflammatory bowel disease surgery
Abstract
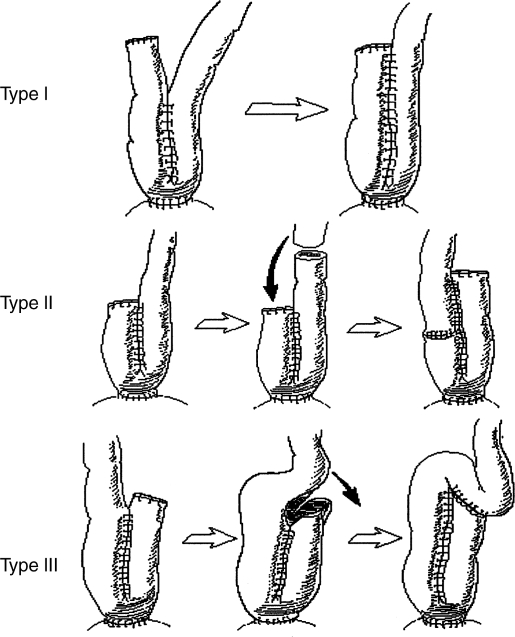
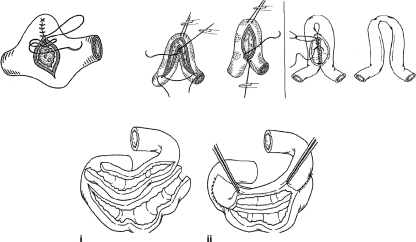
With the advent of restorative proctocolectomy or ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC), not only has there been potential for cure of UC but also patients have enjoyed marked improvements in bowel function, continence, and quality of life. However, IPAA can be complicated by postoperative small bowel obstruction, disease recurrence, and pouch failure secondary to pelvic sepsis, pouch dysfunction, mucosal inflammation, and neoplastic transformation. These may necessitate emergent or expeditious elective reoperation to salvage the pouch and preserve adequate function. Local, transanal, and transabdominal approaches to IPAA salvage are described, and their indications, outcomes, and the clinical parameters that affect the need for salvage are discussed. Pouch excision for failed salvage reoperation is reviewed as well. Relaparotomy is also frequently required for recurrent Crohn's disease (CD), especially given the nature of this as yet incurable illness. Risk factors for CD recurrence are examined, and the various surgical options and margins of resection are evaluated with a focus on bowel-sparing policy. Stricturoplasty, its outcomes, and its importance in recurrent disease are discussed, and segmental resection is compared with more extensive procedures such as total colectomy with ileorectal anastomosis. Lastly, laparoscopy is addressed with respect to its long-term outcomes, effect on surgical recurrence, and its application in the management of recurrent CD.
Keywords: Restorative proctocolectomy; pouch failure; recurrent Crohn's disease; salvage/reoperation; ulcerative colitis.
Figures
References
-
- Corman M. Colon and Rectal Surgery. 5th ed. Philadelphia: Lippincott, Williams, & Wilkins; 2004. pp. 1319–1535.
-
- Penner R, Madsen K, Fedorak R. Postoperative Crohn's disease. Inflamm Bowel Dis. 2005;11:765–777. - PubMed
