

Evaluation of anal incontinence: minimal approach, maximal effectiveness
- PMID: 20011334
- PMCID: PMC2780134
- DOI: 10.1055/s-2005-864076
Evaluation of anal incontinence: minimal approach, maximal effectiveness
Abstract
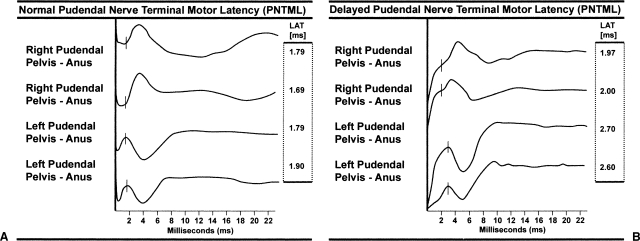
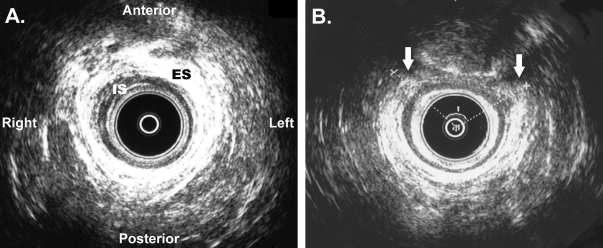
Anal incontinence is a symptom represented by the impaired ability to control the elimination of gas and stool, with an estimated incidence of 2.2 to 7.1% of the population. These numbers likely under-represent the true prevalence because physicians and patients are reluctant to discuss this problem. Evaluation of the patient with anal incontinence requires a fundamental knowledge of the etiologic factors. Careful history and physical examination is essential in every patient and can identify the cause of most cases of incontinence. Incontinence scoring systems are tools that provide objective data regarding the severity and quality of anal incontinence. Supplemental special tests for evaluating incontinence should be aimed at achieving three goals: (1) provide additional and confirmatory information regarding the diagnosis and cause of incontinence; (2) select appropriate treatment; and (3) predict treatment outcome. Numerous studies to evaluate anal incontinence exist; however, the most useful tests to achieve these goals are anal manometry, pudendal nerve terminal motor latency, and anal endosonography, because these studies can identify physiologic, neurologic, and anatomic abnormalities of the anorectum for which there may be effective treatments.
Keywords: Anal; evaluation; fecal; incontinence.
Figures
Similar articles
-
Evaluating patients with anorectal incontinence.Surg Today. 2004;34(4):304-12. doi: 10.1007/s00595-003-2704-2. Surg Today. 2004. PMID: 15052443 Review.
-
Anal endosonography: relationship with anal manometry and neurophysiologic tests.Dis Colon Rectum. 1992 Oct;35(10):944-9. doi: 10.1007/BF02253496. Dis Colon Rectum. 1992. PMID: 1395981
-
Anal continence after rectocele repair.Dis Colon Rectum. 2002 Jan;45(1):63-9. doi: 10.1007/s10350-004-6115-2. Dis Colon Rectum. 2002. PMID: 11786766
-
Pudendal nerve latency. Does it predict outcome of anal sphincter repair?Dis Colon Rectum. 1998 Aug;41(8):1005-9. doi: 10.1007/BF02237391. Dis Colon Rectum. 1998. PMID: 9715157
-
Anorectal incontinence. pathogenesis and choice of treatment.J Gastrointestin Liver Dis. 2006 Mar;15(1):41-9. J Gastrointestin Liver Dis. 2006. PMID: 16680232 Review.
Cited by
-
Survey of anal sphincter dysfunction using anal manometry in patients with fecal incontinence: a possible guide to therapy.Ann Gastroenterol. 2015 Oct-Dec;28(4):469-74. Ann Gastroenterol. 2015. PMID: 26423466 Free PMC article.
-
Bowel management for the treatment of pediatric fecal incontinence.Pediatr Surg Int. 2009 Dec;25(12):1027-42. doi: 10.1007/s00383-009-2502-z. Epub 2009 Oct 15. Pediatr Surg Int. 2009. PMID: 19830436 Free PMC article. Review.
-
Establishing a peripartum perineal trauma clinic: a narrative review.Int Urogynecol J. 2021 Jul;32(7):1653-1662. doi: 10.1007/s00192-020-04631-8. Epub 2021 Jan 5. Int Urogynecol J. 2021. PMID: 33399903 Review.
-
Beyond the numbers: Impact of obesity on obstetric anal sphincter injury (OASI) outcomes in women.Int J Gynaecol Obstet. 2025 Mar;168(3):1171-1177. doi: 10.1002/ijgo.15981. Epub 2024 Oct 21. Int J Gynaecol Obstet. 2025. PMID: 39429224 Free PMC article.
References
-
- Johanson J F, Lafferty J. Epidemiology of fecal incontinence: the silent affliction. Am J Gastroenterol. 1996;91:33–36. - PubMed
-
- Enck P, Bielefeldt K, Rathmann W, Purrmann J, Tschope D, Erckenbrecht J F. Epidemiology of faecal incontinence in selected patient groups. Int J Colorectal Dis. 1991;6:143–146. - PubMed
-
- Nelson R, Norton N, Cautley E, Furner S. Community-based prevalence of anal incontinence. JAMA. 1995;274:559–561. - PubMed
-
- Drossman D A, Li Z, Andruzzi E, et al. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci. 1993;38:1569–1580. - PubMed
-
- Nelson R, Furner S, Jesudason V. Fecal incontinence in Wisconsin nursing homes: prevalence and associations. Dis Colon Rectum. 1998;41:1226–1229. - PubMed
