

doi: 10.1055/s-2007-977486.
Pilonidal disease
Affiliations
- PMID: 20011382
- PMCID: PMC2780177
- DOI: 10.1055/s-2007-977486
Item in Clipboard
Pilonidal disease
Clin Colon Rectal Surg.
2007 May.
Abstract
Pilonidal disease is a common anorectal problem that typically affects young people. Numerous surgical procedures have been described, but treatment failure and disease recurrence are frequent, leading to considerable morbidity in these otherwise healthy patients. To manage this problem successfully, surgeons must consider the pathogenesis and presentation of the disease and weigh the advantages and disadvantages of any operation. Discussed in this article are the pathogenesis of pilonidal disease and basic treatment options for acute pilonidal abscesses, sinus tracts, and chronic or recurrent pilonidal disease.
Keywords: Pilonidal; pathogenesis; review; treatment.
Figures
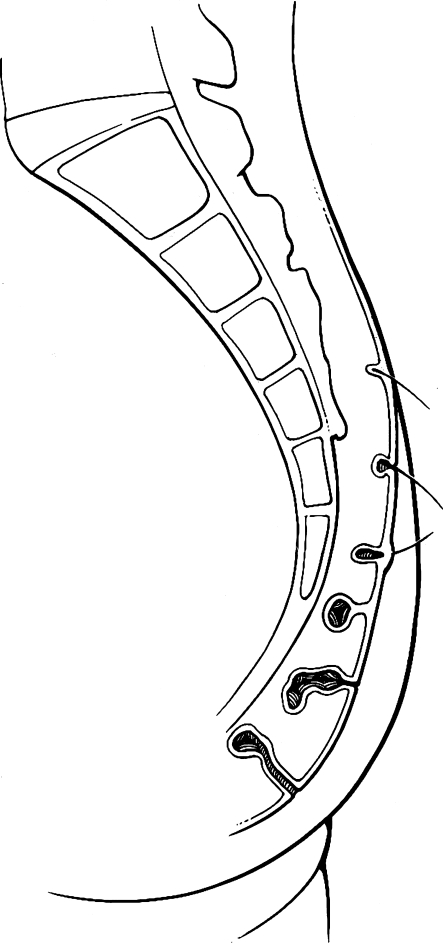
Pathogenesis. Hair invading skin at the natal cleft causes a pilonidal abscess and sinus tracts. Figure used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.
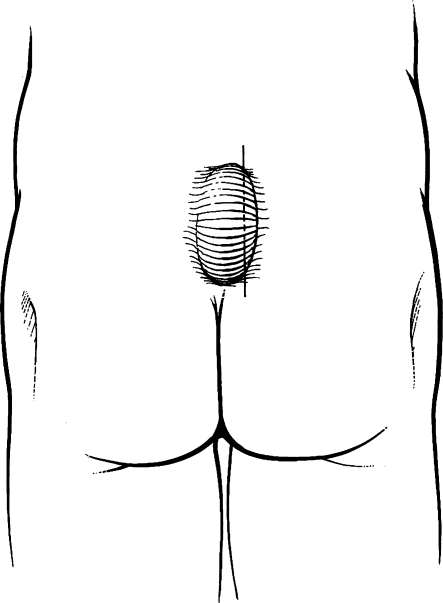
Incision and drainage. The incision should be made lateral to midline. Figure used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.
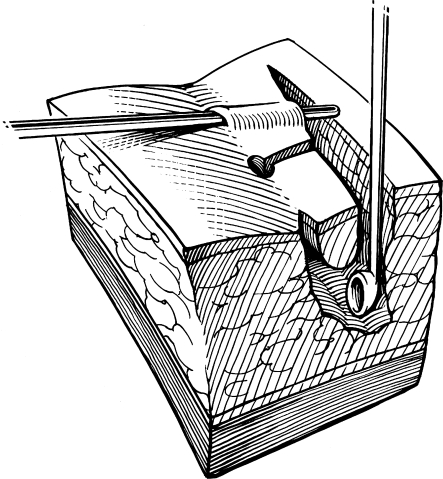
Incision and drainage. Midline pits and sinus tracts are laid open toward the lateral incision, and the cavity is curetted. Figure used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.

Marsupialization. The skin edge is sutured to the base of the wound. Figure used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.
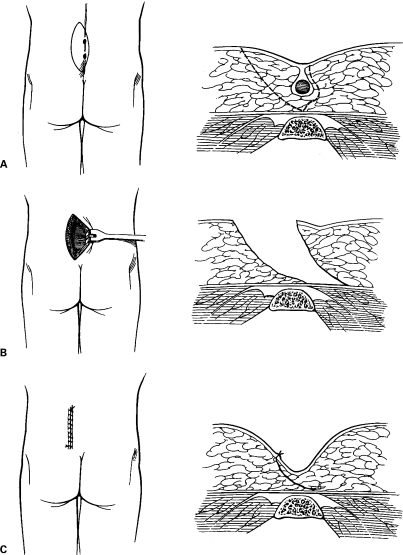
Karydakis procedure. (A) An asymmetric elliptical incision is carried down to the postsacral fascia. (B) The wound is undermined and (C) closed off midline. Figures used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.
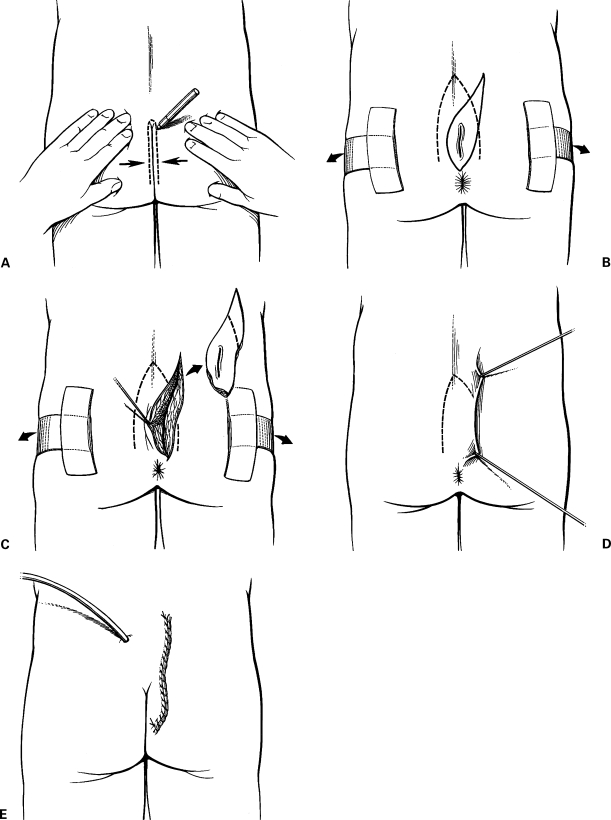
Cleft closure. (A) The line of contact between the buttocks is marked. (B) The buttocks are taped apart and an asymmetric elliptical incision is drawn around the unhealed midline wound. (C) The incision is carried into the subcutaneous fat to wedge out the unhealed wound. (D) A dermal flap is raised, undermining the skin to the marked line of contact. (E) The skin flap is closed over a suction drain. Figures used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.
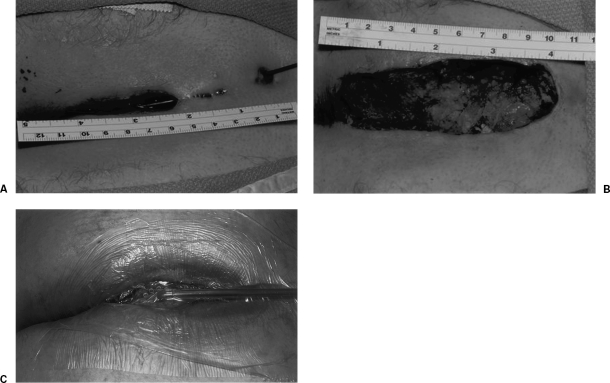
Negative pressure wound therapy. (A) Complex pilonidal disease. (B) Excision of all involved tissue. (C) Primary V.A.C. device placement. Figures used by permission of Mayo Foundation for Medical Education and Research. All rights reserved.
Similar articles
-
Using negative pressure wound therapy following surgery for complex pilonidal disease: a case series.Ostomy Wound Manage. 2007 May;53(5):40-6. Ostomy Wound Manage. 2007. PMID: 17551174
-
[Surgical treatment of pilonidal disease].Tidsskr Nor Laegeforen. 2010 May 6;130(9):936-9. doi: 10.4045/tidsskr.09.0345. Tidsskr Nor Laegeforen. 2010. PMID: 20453956 Review. Norwegian.
-
Modified Bascom's asymmetric midgluteal cleft closure technique for recurrent pilonidal disease: early experience in a military hospital.Dis Colon Rectum. 2003 Sep;46(9):1286-91. doi: 10.1007/s10350-004-6729-4. Dis Colon Rectum. 2003. PMID: 12972977
-
Infrequent Presentation of Pilonidal Sinus over the Nasal Bridge.Indian J Otolaryngol Head Neck Surg. 2024 Feb;76(1):1153-1156. doi: 10.1007/s12070-023-04191-5. Epub 2023 Sep 2. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 38440473 Free PMC article.
-
Disease that should be remembered: Sacrococcygeal pilonidal sinus disease and short history.World J Clin Cases. 2015 Oct 16;3(10):876-9. doi: 10.12998/wjcc.v3.i10.876. World J Clin Cases. 2015. PMID: 26488023 Free PMC article. Review.
Cited by
-
Karydakis procedure for sacrococcygeal pilonidal sinus disease: Our experience.Indian J Plast Surg. 2014 Sep-Dec;47(3):402-6. doi: 10.4103/0970-0358.146615. Indian J Plast Surg. 2014. PMID: 25593428 Free PMC article.
-
Endoscopic pilonidal sinus treatment: a systematic review and meta-analysis.Surg Endosc. 2018 Sep;32(9):3754-3762. doi: 10.1007/s00464-018-6157-5. Epub 2018 Mar 30. Surg Endosc. 2018. PMID: 29603009
-
Horseshoe abscesses in primary care.Can Fam Physician. 2019 Jul;65(7):476-478. Can Fam Physician. 2019. PMID: 31300429 Free PMC article. No abstract available.
-
Pilonidal sinus involving the nasal bridge: a rare manifestation.BMJ Case Rep. 2015 Jul 6;2015:bcr2015209948. doi: 10.1136/bcr-2015-209948. BMJ Case Rep. 2015. PMID: 26150636 Free PMC article.
-
Pilonidal sinus: a comparative study of treatment methods.J Med Life. 2014 Mar 15;7(1):27-30. Epub 2014 Mar 25. J Med Life. 2014. PMID: 24653753 Free PMC article.
References
-
- da Silva J H. Pilonidal cyst. Cause and treatment. Dis Colon Rectum. 2000;43:1146–1156. - PubMed
-
- Bascom J. Pilonidal disease: origin from follicles of hairs and results of follicle removal as treatment. Surgery. 1980;87:567–572. - PubMed
-
- Franckowiak J J, Jackman R J. The etiology of pilonidal sinus. Dis Colon Rectum. 1962;5:28–36. - PubMed
-
- Hardaway R M. Pilonidal cyst—neither pilonidal nor cyst. Arch Surg. 1958;76:143–147. - PubMed
-
- Sondenaa K, Nesvik I, Anderson E, Natas O, Soreide J A. Patient characteristics and symptoms in chronic pilonidal sinus disease. Int J Colorectal Dis. 1995;10:39–42. - PubMed
